Stem Cell and Gene Therapy Program, Fred Hutchinson Cancer Research Center, Seattle, WA.
Boston Children's Hospital/Dana-Farber Cancer Institute-Department of Pediatrics, Harvard Medical School, Boston, MA.
Blood. 2020 Oct 8;136(15):1722-1734. doi: 10.1182/blood.2020006372.
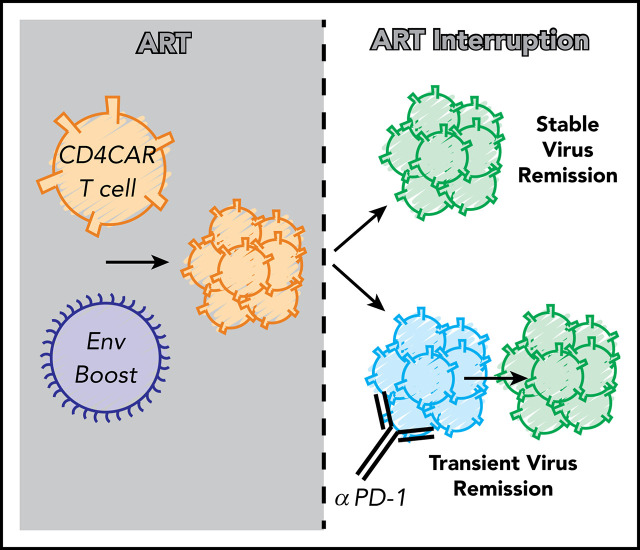
Chimeric antigen receptor (CAR) T cells targeting CD19+ hematologic malignancies have rapidly emerged as a promising, novel therapy. In contrast, results from the few CAR T-cell studies for infectious diseases such as HIV-1 have been less convincing. These challenges are likely due to the low level of antigen present in antiretroviral therapy (ART)-suppressed patients in contrast to those with hematologic malignancies. Using our well-established nonhuman primate model of ART-suppressed HIV-1 infection, we tested strategies to overcome these limitations and challenges. We first optimized CAR T-cell production to maintain central memory subsets, consistent with current clinical paradigms. We hypothesized that additional exogenous antigen might be required in an ART-suppressed setting to aid expansion and persistence of CAR T cells. Thus, we studied 4 simian/HIV-infected, ART-suppressed rhesus macaques infused with virus-specific CD4CAR T cells, followed by supplemental infusion of cell-associated HIV-1 envelope (Env). Env boosting led to significant and unprecedented expansion of virus-specific CAR+ T cells in vivo; after ART treatment interruption, viral rebound was significantly delayed compared with controls (P = .014). In 2 animals with declining CAR T cells, rhesusized anti-programmed cell death protein 1 (PD-1) antibody was administered to reverse PD-1-dependent immune exhaustion. Immune checkpoint blockade triggered expansion of exhausted CAR T cells and concordantly lowered viral loads to undetectable levels. These results show that supplemental cell-associated antigen enables robust expansion of CAR T cells in an antigen-sparse environment. To our knowledge, this is the first study to show expansion of virus-specific CAR T cells in infected, suppressed hosts, and delay/control of viral recrudescence.
嵌合抗原受体 (CAR) T 细胞靶向 CD19+血液系统恶性肿瘤已迅速成为一种有前途的新型疗法。相比之下,针对 HIV-1 等传染病的 CAR T 细胞研究结果则不那么令人信服。这些挑战可能是由于接受抗逆转录病毒治疗 (ART)抑制的患者体内抗原水平较低,与血液系统恶性肿瘤患者相比。我们使用经过充分验证的非人类灵长类动物模型进行了抗逆转录病毒治疗抑制的 HIV-1 感染研究,以测试克服这些限制和挑战的策略。我们首先优化了 CAR T 细胞的生产工艺,以维持符合当前临床模式的中央记忆亚群。我们假设在抗逆转录病毒治疗抑制的环境中,可能需要额外的外源性抗原来帮助 CAR T 细胞的扩增和持续存在。因此,我们研究了 4 只感染 simian/HIV、接受抗逆转录病毒治疗抑制的恒河猴,给它们输注了病毒特异性 CD4CAR T 细胞,随后补充输注了细胞相关的 HIV-1 包膜 (Env)。Env 增强导致体内病毒特异性 CAR+T 细胞的显著且前所未有的扩增;与对照组相比,在停止 ART 治疗后,病毒反弹明显延迟(P=0.014)。在 2 只 CAR T 细胞数量下降的动物中,给予了恒河猴化抗程序性细胞死亡蛋白 1 (PD-1) 抗体以逆转 PD-1 依赖性免疫衰竭。免疫检查点阻断触发了耗尽的 CAR T 细胞的扩增,并相应地降低了病毒载量至不可检测水平。这些结果表明,补充细胞相关抗原能够在抗原稀少的环境中实现 CAR T 细胞的强大扩增。据我们所知,这是首次在感染和抑制的宿主中显示病毒特异性 CAR T 细胞扩增,并延迟/控制病毒复发的研究。