Department of Medicine, Division of Hospice and Palliative Care, North Shore University Hospital, Manhasset, NY, USA.
Department of Medicine, Division of Hematology and Oncology, State University New York (SUNY) Downstate Medical Center, Brooklyn, NY, USA.
Am J Case Rep. 2020 Jul 3;21:e924798. doi: 10.12659/AJCR.924798.
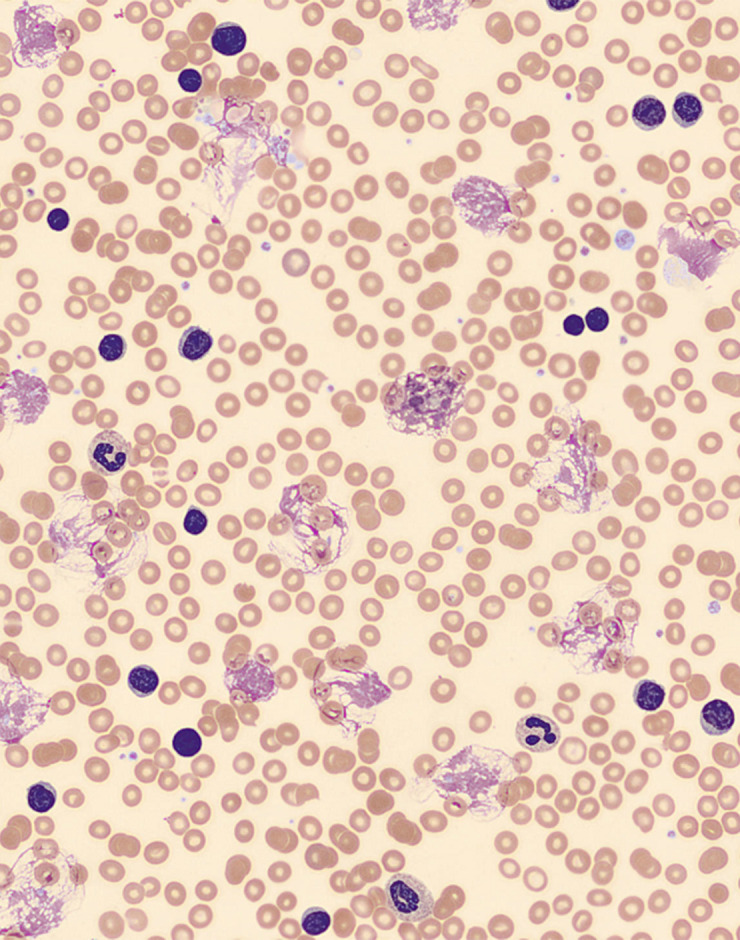
BACKGROUND Chronic lymphocytic leukemia (CLL) is a mature B cell lymphocytic neoplasm that has an indolent clinical course. Therefore, not all patients with CLL require treatment at the time of diagnosis. Hyperleukocytosis (white blood cell count, >100×10⁹/L) is present in a large proportion of patients with CLL. However, symptomatic hyperleukocytosis (leukostasis) is an extremely uncommon presentation of CLL. Leukostasis frequently presents with the clinical manifestation of respiratory, neurological, or renal system problems. This is secondary to the decreased tissue perfusion due to the intravascular accumulation of large aggregates of leukemic cells. Leukostasis is a medical emergency requiring intensive care unit (ICU) admission and its management includes aggressive hydration, prevention and treatment of tumor lysis syndrome, cytoreduction, and leukapheresis. CASE REPORT We report a case of a 77-year-old woman with a long history of untreated CLL who presented with respiratory symptoms with hyperleukocytosis. Her condition rapidly deteriorated, requiring intubation. She required induction chemotherapy with chlorambucil as well as 2 sessions of leukapheresis, to which she responded well. In most reported leukostasis cases in the literature, the white blood cell (WBC) count was >1000×10⁹/L. We present a case of a patient with leukostasis with WBC count 524×10⁹/L who responded to chlorambucil and leukapheresis, with good recovery. CONCLUSIONS Leukostasis, although extremely rare, is a life-threatening complication in patients with CLL. It should be strongly considered in the differential diagnosis of patients with CLL who present with hyperleukocytosis and acute pulmonary symptoms. Clinicians should be aware of this medical emergency, as delayed treatment can increase morbidity and mortality.
慢性淋巴细胞白血病(CLL)是一种成熟 B 细胞淋巴细胞肿瘤,具有惰性的临床病程。因此,并非所有 CLL 患者在诊断时都需要治疗。大多数 CLL 患者存在白细胞增多(白细胞计数>100×10⁹/L)。然而,有症状的白细胞增多(白细胞淤滞)是 CLL 极为罕见的表现。白细胞淤滞常表现为呼吸系统、神经系统或肾脏系统问题的临床表现。这是由于大量白血病细胞在血管内积聚导致组织灌注减少所致。白细胞淤滞是一种需要入住重症监护病房(ICU)的医疗紧急情况,其治疗包括积极水化、预防和治疗肿瘤溶解综合征、细胞减少和白细胞去除。
我们报告了一例 77 岁女性患有长期未经治疗的 CLL,表现为白细胞增多伴呼吸症状。她的病情迅速恶化,需要插管。她需要接受苯丁酸氮芥诱导化疗以及 2 次白细胞去除术,对这些治疗她反应良好。在文献中报道的大多数白细胞淤滞病例中,白细胞(WBC)计数>1000×10⁹/L。我们报告了一例白细胞淤滞患者,WBC 计数为 524×10⁹/L,对苯丁酸氮芥和白细胞去除术有反应,恢复良好。
尽管白细胞淤滞极为罕见,但它是 CLL 患者危及生命的并发症。对于白细胞增多和急性肺部症状的 CLL 患者,应强烈考虑这种并发症。临床医生应意识到这种医疗紧急情况,因为延迟治疗会增加发病率和死亡率。