Implementation Science Unit, Centre for Infectious Disease Research in Zambia (CIDRZ), Lusaka, Zambia.
Division of Infectious Diseases, School of Medicine, Washington University, St. Louis, MO, USA.
J Int AIDS Soc. 2020 Jul;23(7):e25560. doi: 10.1002/jia2.25560.
In the current "test and treat" era, HIV programmes are increasingly focusing resources on linkage to care and same-day antiretroviral therapy (ART) initiation to meet UNAIDS 95-95-95 targets. After observing sub-optimal treatment indicators in health facilities supported by the Centre for Infectious Disease Research in Zambia (CIDRZ), we piloted a "linkage assessment" tool in facility-based HIV testing settings to uncover barriers to same-day linkage to care and ART initiation among newly identified people living with HIV (PLHIV) and to guide HIV programme quality improvement efforts.
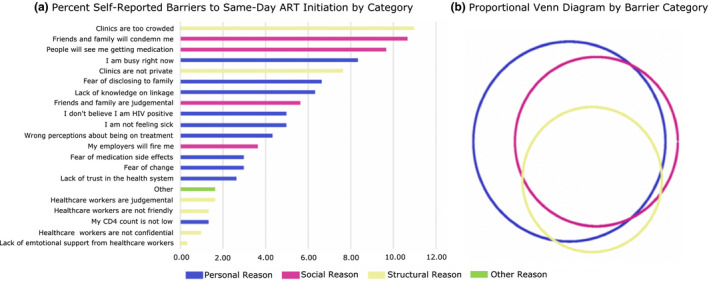
The one-page, structured linkage assessment tool was developed to capture patient-reported barriers to same-day linkage and ART initiation using three empirically supported categories of barriers: social, personal and structural. The tool was implemented in three health facilities, two urban and one rural, in Lusaka, Zambia from 1 November 2017 to 31 January 2018, and administered to all newly identified PLHIV declining same-day linkage and ART. Individuals selected as many reasons as relevant. We used mixed-effects logistic regression modelling to evaluate predictors of citing specific barriers to same-day linkage and ART, and Fisher's Exact tests to assess differences in barrier citation by socio-demographics and HIV testing entry point.
A total of 1278 people tested HIV positive, of whom 126 (9.9%) declined same-day linkage and ART, reporting a median of three barriers per respondent. Of these 126, 71.4% were female. Females declining same-day ART were younger, on average, (median 28.5 years, interquartile range (IQR): 21 to 37 years) than males (median 34.5 years, IQR: 26 to 44 years). The most commonly reported barrier category was structural, "clinics were too crowded" (n = 33), followed by a social reason, "friends and family will condemn me" (n = 30). The frequency of citing personal barriers differed significantly across HIV testing point (χ p = 0.03). Significant predictors for citing ≥1 barrier to same-day ART were >50 years of age (OR: 12.59, 95% CI: 6.00 to 26.41) and testing at a rural facility (OR: 9.92, 95% CI: 4.98 to 19.79).
Given differences observed in barriers to same-day ART initiation reported across sex, age, testing point, and facility type, new, tailored counselling and linkage to care approaches are needed, which should be rigorously evaluated in routine programme settings.
在当前的“检测即治疗”时代,艾滋病毒规划越来越多地将资源集中用于建立联系以提供护理和当天开始抗逆转录病毒治疗(ART),以实现联合国艾滋病规划署 95-95-95 目标。在观察到赞比亚传染病研究中心(CIDRZ)支持的卫生机构的治疗指标欠佳后,我们在基于机构的艾滋病毒检测环境中试用了一种“联系评估”工具,以发现新确诊的艾滋病毒感染者(PLHIV)当天建立联系以获得护理和开始接受抗逆转录病毒治疗方面的障碍,并指导艾滋病毒规划质量改进工作。
该单页结构化联系评估工具用于使用经验证的三个障碍类别来捕获患者报告的当天建立联系和开始 ART 的障碍:社会、个人和结构。该工具于 2017 年 11 月 1 日至 2018 年 1 月 31 日在赞比亚卢萨卡的三个卫生机构中实施,其中两个是城市机构,一个是农村机构,用于对所有新确诊的拒绝当天建立联系和开始 ART 的 PLHIV 进行评估。个人选择尽可能多的相关原因。我们使用混合效应逻辑回归模型来评估对当天建立联系和开始 ART 提出具体障碍的预测因素,并使用 Fisher 精确检验来评估社会人口统计学特征和 HIV 检测切入点的障碍引用差异。
共有 1278 人检测出艾滋病毒呈阳性,其中 126 人(9.9%)拒绝当天建立联系并开始接受 ART,每位受访者报告的中位数为三个障碍。在这 126 人中,71.4%为女性。拒绝当天接受 ART 的女性平均年龄较小(中位数 28.5 岁,四分位距(IQR):21 至 37 岁),而男性(中位数 34.5 岁,IQR:26 至 44 岁)。最常报告的障碍类别是结构性的,“诊所太拥挤”(n=33),其次是社会原因,“朋友和家人会谴责我”(n=30)。在不同的 HIV 检测点,个人障碍的引用频率存在显著差异(χ p=0.03)。当天开始 ART 引用≥1 个障碍的显著预测因素是年龄>50 岁(OR:12.59,95%CI:6.00 至 26.41)和在农村机构检测(OR:9.92,95%CI:4.98 至 19.79)。
鉴于在性、年龄、检测点和机构类型方面报告的当天开始 ART 障碍方面观察到的差异,需要采取新的、有针对性的咨询和联系护理方法,并应在常规规划环境中对其进行严格评估。