Health Action International, Overtoom 60-2, 1054, HK, Amsterdam, The Netherlands.
WHO Collaborating Centre for Pharmaceutical Policy and Regulation, Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences (UIPS), Utrecht University, Utrecht, The Netherlands.
BMC Public Health. 2020 Jul 3;20(1):1053. doi: 10.1186/s12889-020-09155-w.
Access to sexual and reproductive health services continues to be a public health concern in Kenya, Tanzania, Uganda and Zambia: use of modern contraceptives is low, and unmet family planning needs and maternal mortality remain high. This study is an assessment of the availability, affordability and stock-outs of essential sexual and reproductive health commodities (SRHC) in these countries to inform interventions to improve access.
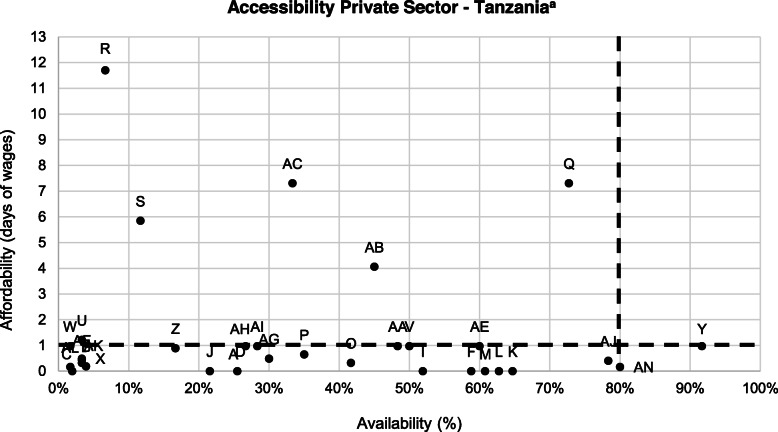
The study consisted of an adaptation of the World Health Organization/Health Action International methodology, Measuring Medicine Prices, Availability, Affordability and Price Components. Price, availability and stock-out data was collected in July 2019 for over fifty lowest-priced SRHC from public, private and private not-for-profit health facilities in Kenya (n = 221), Tanzania (n = 373), Uganda (n = 146) and Zambia (n = 245). Affordability was calculated using the wage of a lowest-paid government worker. Accessibility was illustrated by combining the availability (≥ 80%) and affordability (less than 1 day's wage) measures.
Overall availability of SRHC was low at less than 50% in all sectors, areas and countries, with highest mean availability found in Kenyan public facilities (46.6%). Stock-outs were common; the average number of stock-out days per month ranged from 3 days in Kenya's private and private not-for-profit sectors, to 12 days in Zambia's public sector. In the public sectors of Kenya, Uganda and Zambia, as well as in Zambia's private not-for-profit sector, all SRHC were free for the patient. In the other sectors unaffordability ranged from 2 to 9 SRHC being unaffordable, with magnesium sulphate being especially unaffordable in the countries. Accessibility was low across the countries, with Kenya's and Zambia's public sectors having six SRHC that met the accessibility threshold, while the private sector of Uganda had only one SRHC meeting the threshold.
Accessibility of SRHC remains a challenge. Low availability of SRHC in the public sector is compounded by regular stock-outs, forcing patients to seek care in other sectors where there are availability and affordability challenges. Health system strengthening is needed to ensure access, and these findings should be used by national governments to identify the gaps and shortcomings in their supply chains.
在肯尼亚、坦桑尼亚、乌干达和赞比亚,获得性和生殖健康服务的途径仍然是公共卫生关注的一个问题:现代避孕药具的使用率较低,计划生育需求未得到满足,孕产妇死亡率仍然很高。本研究评估了这些国家基本性和生殖健康商品(SRHC)的供应、可负担性和缺货情况,以了解干预措施以改善获得途径。
该研究改编自世界卫生组织/健康行动国际组织的方法,即衡量药品价格、供应、可负担性和价格构成。2019 年 7 月,从肯尼亚(n=221)、坦桑尼亚(n=373)、乌干达(n=146)和赞比亚(n=245)的公立、私立和非营利性私立医疗机构中收集了 50 多种最低价的 SRHC 的价格、供应和缺货数据。使用最低工资政府工人的工资来计算可负担性。通过结合供应(≥80%)和可负担性(不到 1 天的工资)措施来表示可及性。
在所有部门、地区和国家,SRHC 的总体供应率均低于 50%,肯尼亚公立机构的平均供应率最高(46.6%)。缺货情况很常见;每月缺货天数平均为 3 天,肯尼亚的私营和非营利部门,到 12 天,赞比亚的公共部门。在肯尼亚、乌干达和赞比亚的公共部门,以及赞比亚的非营利部门,所有 SRHC 对患者都是免费的。在其他部门,有 2 到 9 种 SRHC 无法负担,其中硫酸镁在这些国家特别难以负担。在这些国家,可及性都很低,肯尼亚和赞比亚的公共部门有 6 种 SRHC 达到了可及性门槛,而乌干达的私营部门只有 1 种 SRHC 达到了门槛。
SRHC 的可及性仍然是一个挑战。公立部门 SRHC 的供应不足加上定期缺货,迫使患者到其他供应和负担能力方面存在挑战的部门寻求治疗。需要加强卫生系统,以确保获得途径,国家政府应利用这些发现来确定其供应链中的差距和缺陷。