Center for Health and Technology, Department of Pediatrics, University of California, Davis, Sacramento.
Center for Healthcare Policy and Research, Department of Pediatrics, University of California, Davis, Sacramento.
JAMA Netw Open. 2020 Jul 1;3(7):e2010174. doi: 10.1001/jamanetworkopen.2020.10174.
Adherence to telemonitoring may be associated with heart failure exacerbation but is not included in telemonitoring algorithms.
To assess whether telemonitoring adherence is associated with a patient's risk of hospitalization, emergency department visit, or death.
DESIGN, SETTING, AND PARTICIPANTS: This post hoc secondary analysis of the Better Effectiveness After Transition-Heart Failure randomized clinical trial included patients from 6 academic medical centers in California who were eligible if they were hospitalized for decompensated heart failure and excluded if they were discharged to a skilled nursing facility, were expected to improve because of a medical procedure, or did not have the cognitive or physical ability to participate. The trial compared a telemonitoring intervention with usual care for patients with heart failure after hospital discharge from October 12, 2011, to September 30, 2013. Data analysis was performed from November 8, 2016, to May 10, 2019.
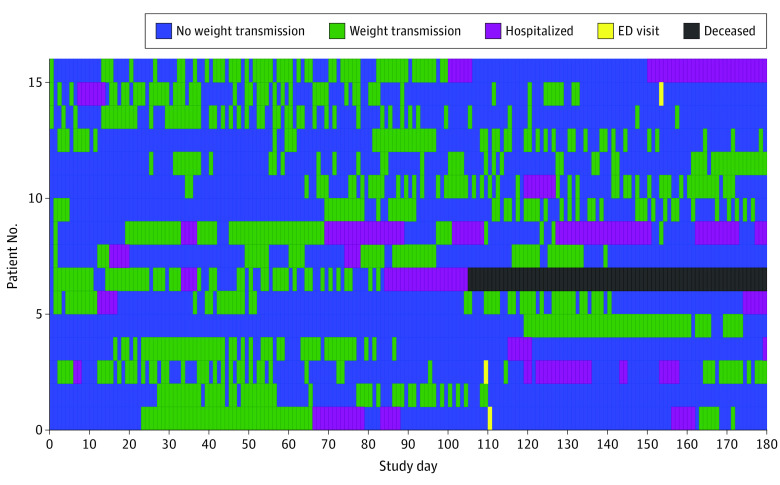
The intervention group (n = 722) received heart failure education, telephone check-ins, and a wireless telemonitoring system that allowed the patient to transmit weight, blood pressure, heart rate, and selected symptoms. The control group (n = 715) received usual care. Patients were followed up for 180 days after discharge.
The main outcome was within-person risk of hospitalization, emergency department visit, or death by week during the study period. Poisson regression was used to determine the within-person association of adherence to daily weighing with the risk of experiencing these events in the following week.
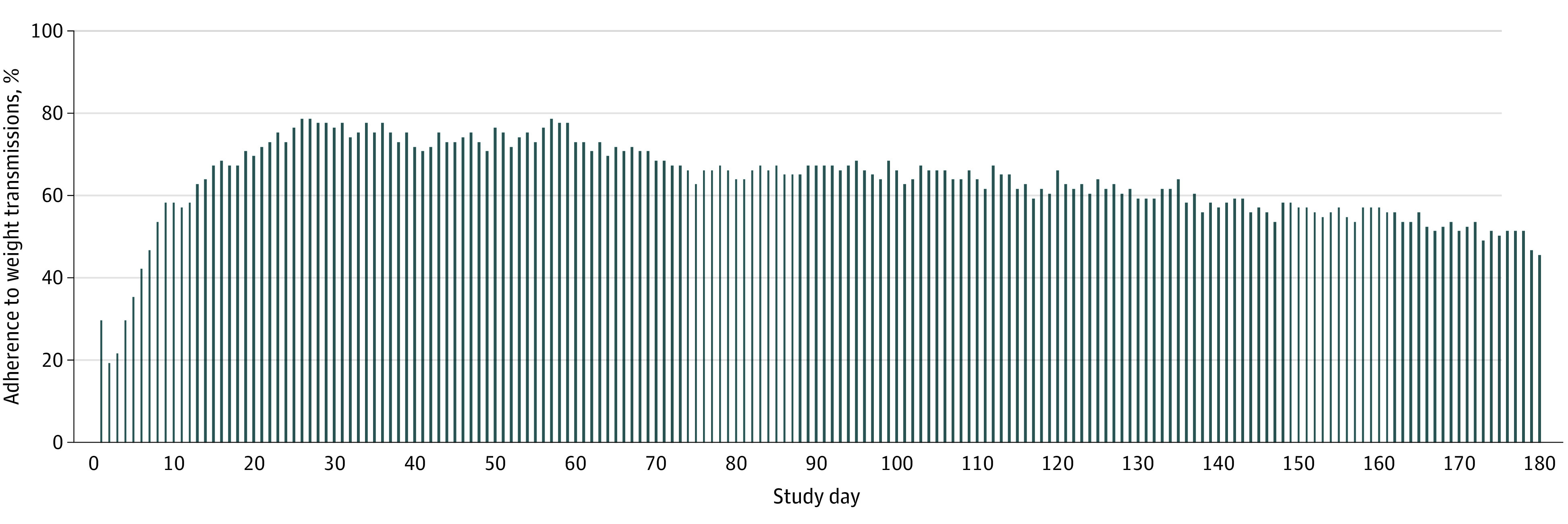
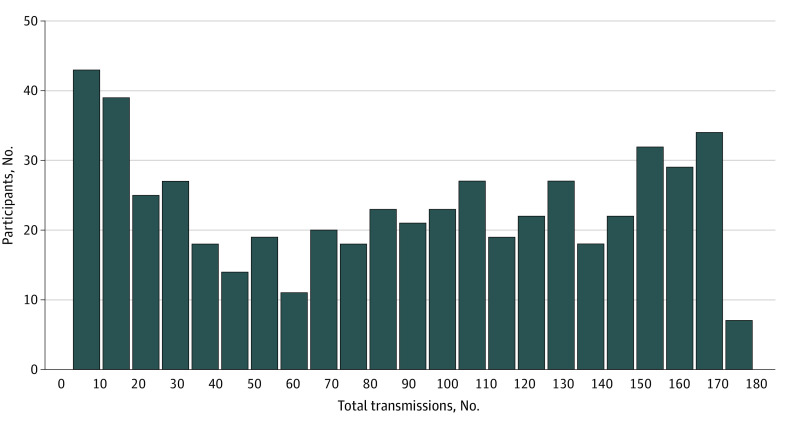
Among the 538 participants (mean [SD] age, 70.9 [14.1] years; 287 [53.8%] male; 269 [50.7%] white) in the present analysis, adherence was lowest during the first week after enrollment but steadily increased, peaking between days 26 and 60 at 69%, or 371 transmissions. Adherence to weight telemonitoring was associated with events in the following week; an increase in adherence by 1 day was associated with a 19% decrease in the rate of death in the following week (incidence rate ratio, 0.81; 95% CI, 0.73-0.90) and an 11% decrease in the rate of hospitalization (incidence rate ratio, 0.89; 95% CI, 0.86-0.91). Adherence in the previous week was not associated with reduced rates of emergency department visits (incidence rate ratio, 0.95; 95% CI, 0.90-1.02).
In this study, lower adherence to weight telemonitoring in a given week was associated with an increased risk of subsequent hospitalization or death in the following week. It is unlikely that this is a result of the telemonitoring intervention; rather, adherence may be an important factor associated with a patient's health status.
对远程监测的依从性可能与心力衰竭恶化有关,但不在远程监测算法中。
评估远程监测的依从性是否与患者住院、急诊就诊或死亡的风险相关。
设计、地点和参与者:这是对加利福尼亚州 6 家学术医疗中心的 Better Effectiveness After Transition-Heart Failure 随机临床试验的事后二次分析,纳入了因失代偿性心力衰竭住院的患者,如果他们出院到熟练护理机构、预计因医疗程序而改善或因认知或身体能力而无法参加,则排除在外。该试验比较了远程监测干预与心力衰竭患者出院后的常规护理,时间为 2011 年 10 月 12 日至 2013 年 9 月 30 日。数据分析于 2016 年 11 月 8 日至 2019 年 5 月 10 日进行。
干预组(n=722)接受心力衰竭教育、电话检查和无线远程监测系统,允许患者传输体重、血压、心率和选定的症状。对照组(n=715)接受常规护理。患者在出院后 180 天内接受随访。
主要结局是在研究期间每周的个体住院、急诊就诊或死亡风险。泊松回归用于确定在接下来的一周内,每天称重的依从性与经历这些事件的风险之间的个体关联。
在本分析中的 538 名参与者(平均[标准差]年龄,70.9[14.1]岁;287[53.8%]男性;269[50.7%]白人)中,依从性在入组后的第一周最低,但稳步上升,在第 26 天至 60 天达到峰值,为 69%或 371 次传输。体重远程监测的依从性与接下来一周的事件相关;依从性增加 1 天与接下来一周死亡率降低 19%相关(发病率比,0.81;95%CI,0.73-0.90)和住院率降低 11%相关(发病率比,0.89;95%CI,0.86-0.91)。前一周的依从性与急诊就诊率降低无关(发病率比,0.95;95%CI,0.90-1.02)。
在这项研究中,给定周内体重远程监测依从性较低与接下来一周内住院或死亡风险增加相关。这不太可能是远程监测干预的结果;相反,依从性可能是与患者健康状况相关的一个重要因素。