Kuster Nils, Huet Fabien, Dupuy Anne-Marie, Akodad Mariama, Battistella Pascal, Agullo Audrey, Leclercq Florence, Kalmanovich Eran, Meilhac Alexandra, Aguilhon Sylvain, Cristol Jean-Paul, Roubille Francois
Department of Biochemistry, Centre Ressources Biologiques de Montpellier, University Hospital of Montpellier, Montpellier, France.
PhyMedExp, University of Montpellier, INSERM U1046, CNRS UMR 9214, Montpellier, France.
ESC Heart Fail. 2020 Oct;7(5):2230-2239. doi: 10.1002/ehf2.12680. Epub 2020 Jul 10.
Inflammation and cardiac remodelling are common and synergistic pathways in heart failure (HF). Emerging biomarkers such as soluble suppression of tumorigenicity 2 (sST2) and growth differentiation factor-15 (GDF-15), which are linked to inflammation and fibrosis process, have been proposed as prognosis factors. However, their potential additive values remain poorly investigated.
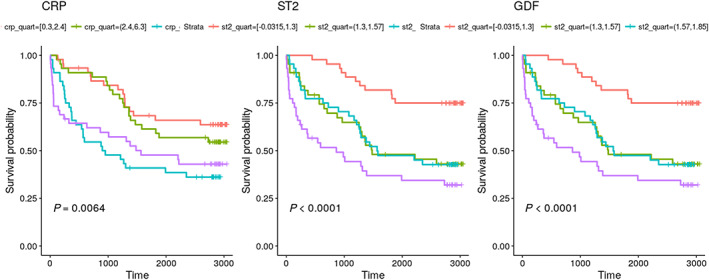
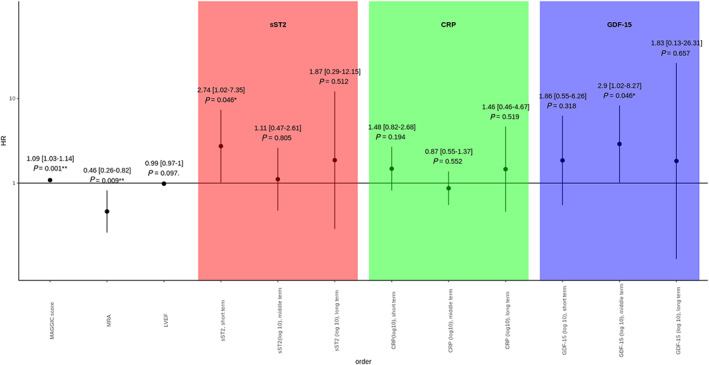
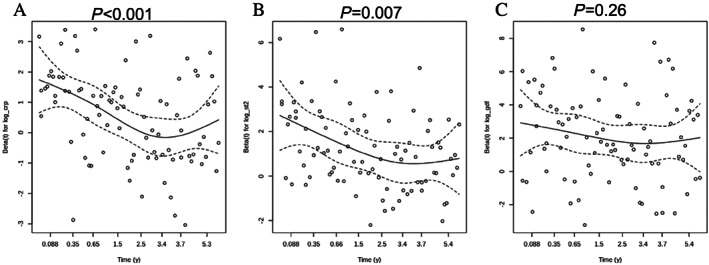
Here, we aimed at evaluating inflammatory and remodelling biomarkers to predict both short-term and long-term mortality in a population with chronic HF in comparison with other classical clinical or biological markers (i.e. N terminal pro brain natriuretic peptide, hs-cTnT, C-reactive protein) alone or using meta-analysis global group in chronic HF risk score in a cohort of 182 patients followed during 80 months (interquartile range: 12.3-90.0). Proportional hazard assumption does not hold for sST2 and C-reactive protein, and follow-up was split into short term (less than 1 year), midterm (between 1 and 5 years), and long term (after 5 years). In univariate analysis, C-reactive protein and sST2 were predictive of short-term mortality but not of middle term and long term whereas GDF-15 was predictive of short and mid-term but not of long-term mortality. In a multivariate model after adjustment for meta-analysis global group in chronic HF score including the three markers, only sST2 was predictive of short-term mortality (P = 0.0225), and only GDF-15 was predictive of middle term mortality (P = 0.0375). None of the markers was predictive of long-term mortality.
Our results demonstrate that both sST2 and GDF-15 significantly improve the prognosis evaluation of HF patients and suggest that the value of GDF-15 is more sustained overtime and could predict middle term events.
炎症和心脏重塑是心力衰竭(HF)常见的协同途径。诸如可溶性肿瘤抑制因子2(sST2)和生长分化因子15(GDF-15)等新兴生物标志物与炎症和纤维化过程相关,已被提议作为预后因素。然而,它们潜在的附加价值仍未得到充分研究。
在此,我们旨在评估炎症和重塑生物标志物,以预测慢性HF患者的短期和长期死亡率,并与其他经典临床或生物学标志物(即N末端脑钠肽前体、高敏肌钙蛋白T、C反应蛋白)单独或在慢性HF风险评分的荟萃分析全局组中进行比较,该队列包括182例患者,随访80个月(四分位间距:12.3 - 90.0)。sST2和C反应蛋白不符合比例风险假设,随访分为短期(少于1年)、中期(1至5年之间)和长期(5年后)。在单变量分析中,C反应蛋白和sST2可预测短期死亡率,但不能预测中期和长期死亡率,而GDF-15可预测短期和中期死亡率,但不能预测长期死亡率。在调整了包括这三种标志物的慢性HF评分的荟萃分析全局组的多变量模型中,只有sST2可预测短期死亡率(P = 0.0225),只有GDF-15可预测中期死亡率(P = 0.0375)。没有一种标志物可预测长期死亡率。
我们的结果表明,sST2和GDF-15均显著改善了HF患者的预后评估,并表明GDF-15的价值在更长时间内更持久,且可预测中期事件。