Fink Ericka L, Wisnowski Jessica, Clark Robert, Berger Rachel P, Fabio Anthony, Furtado Andre, Narayan Srikala, Angus Derek C, Watson R Scott, Wang Chunyan, Callaway Clifton W, Bell Michael J, Kochanek Patrick M, Bluml Stefan, Panigrahy Ashok
Department of Pediatrics, UPMC Children's Hospital of Pittsburgh, Pittsburgh, PA, USA; Department of Critical Care Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA, USA; Safar Center for Resuscitation Research, Pittsburgh, PA, USA.
Children's Hospital of Los Angeles, Los Angeles, CA, USA.
Resuscitation. 2020 Dec;157:185-194. doi: 10.1016/j.resuscitation.2020.06.033. Epub 2020 Jul 9.
Children surviving cardiac arrest are at high risk of neurological morbidity and mortality; however, there is a lack of validated prognostic biomarkers. We aimed to evaluate brain magnetic resonance imaging (MRI) and spectroscopy (MRS) as predictors of death and disability. Secondly, we evaluated whether MRI/S by randomized group.
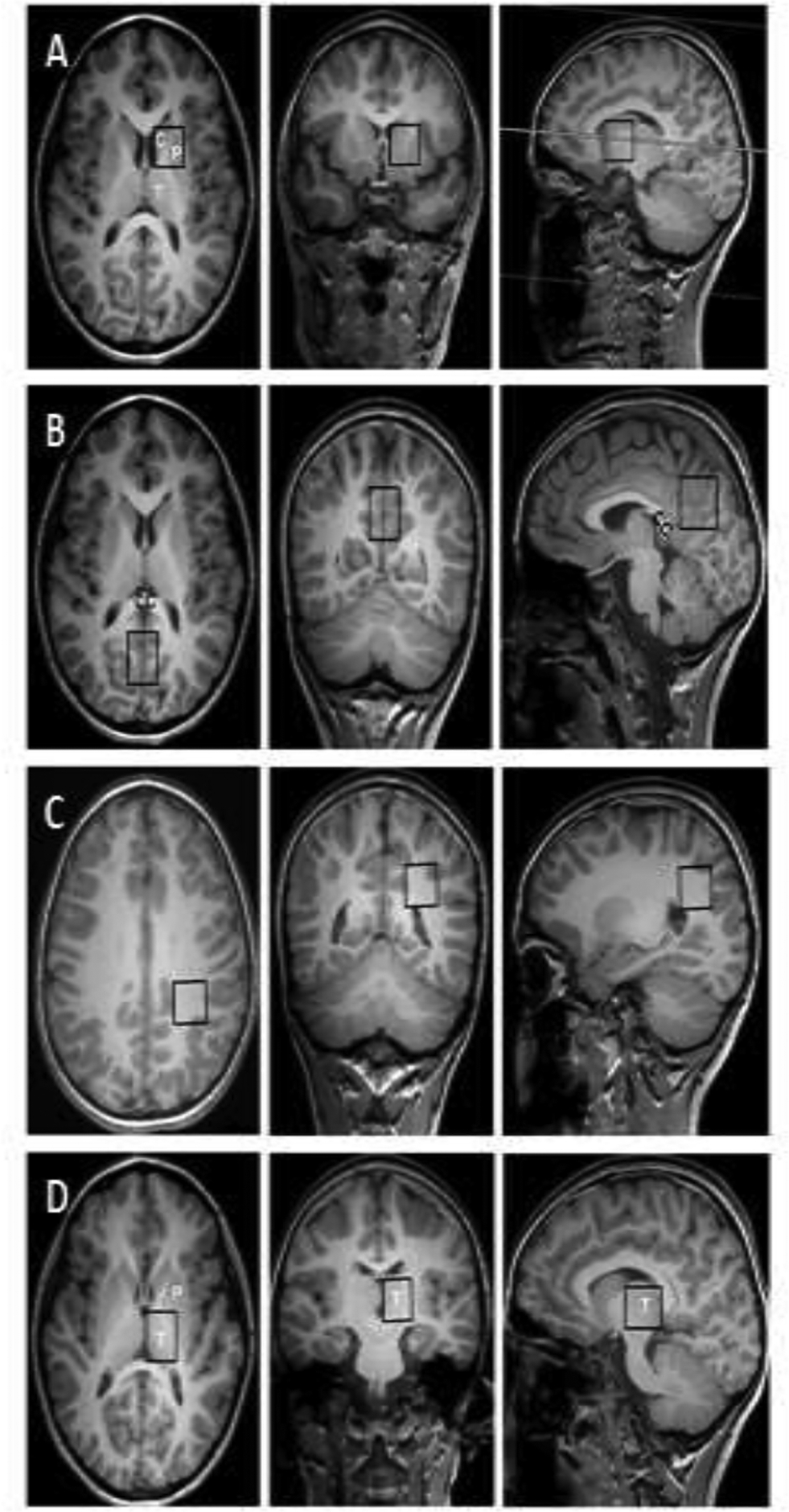
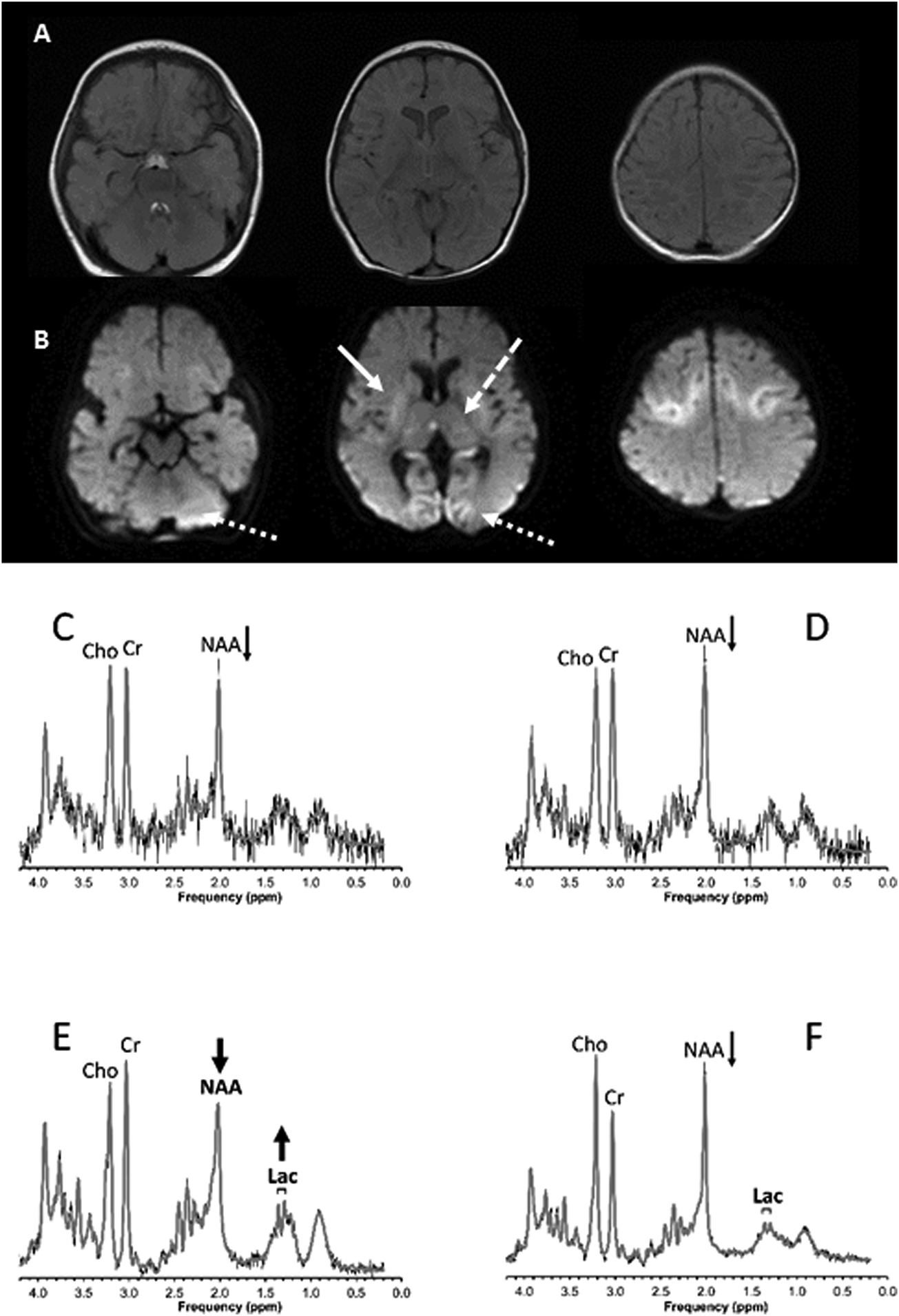
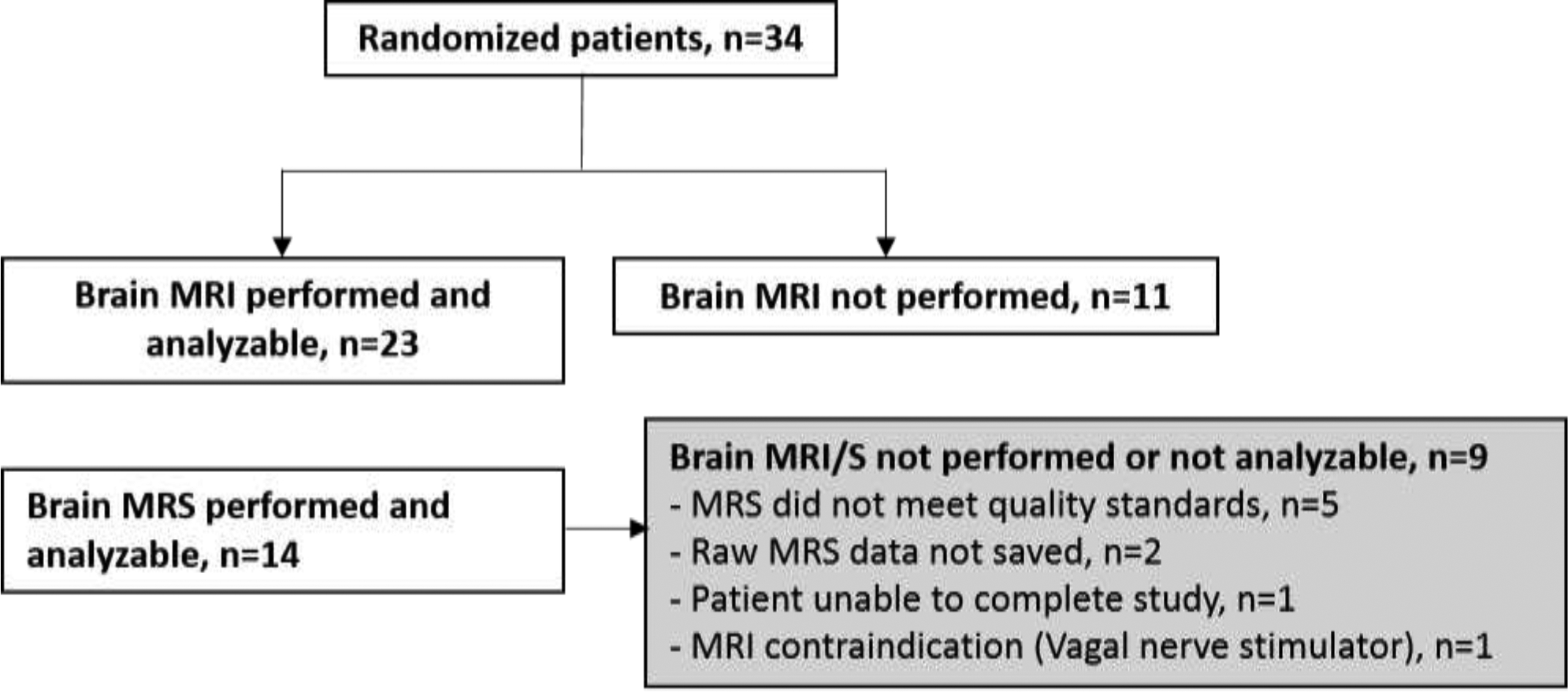
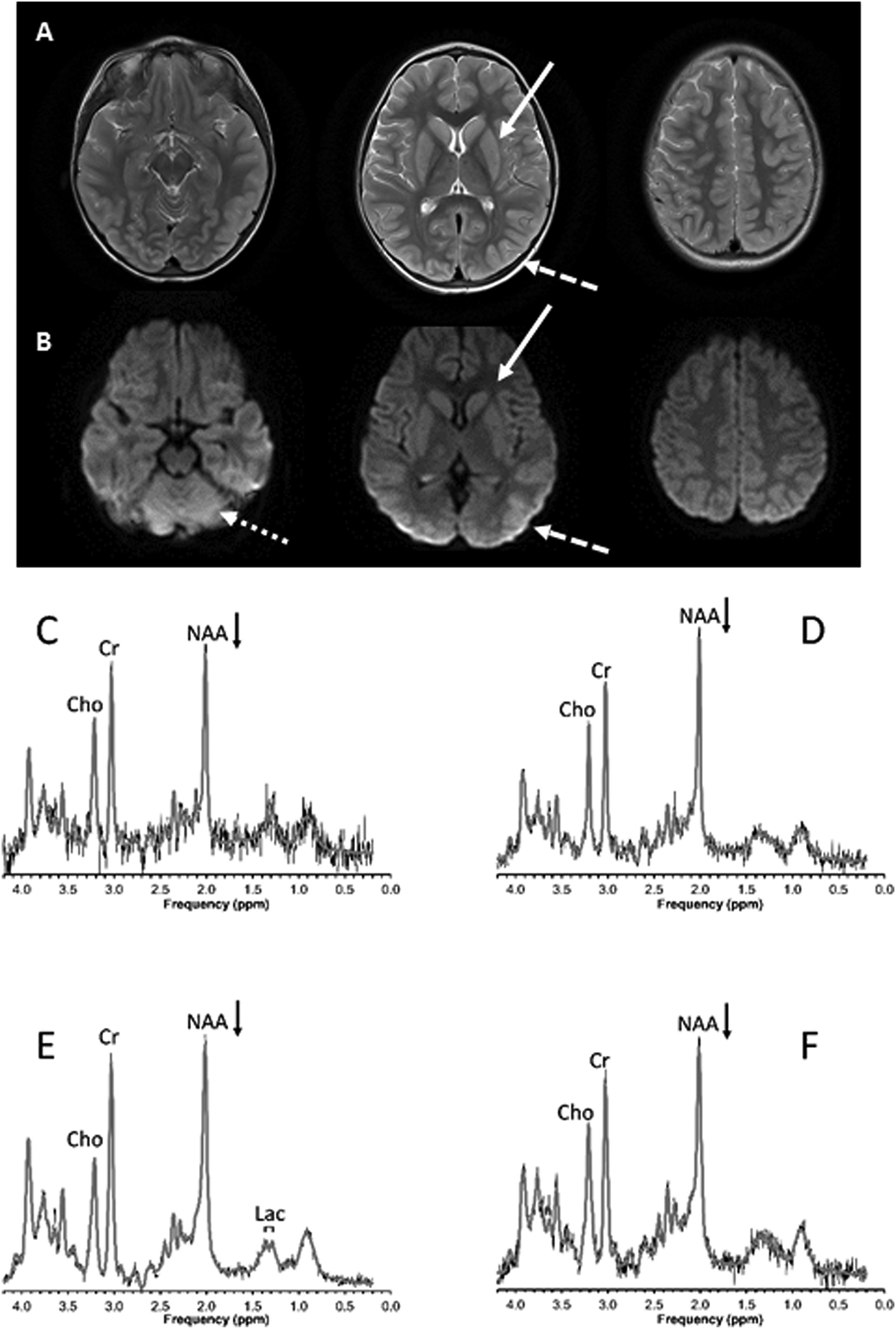
This single center study analyzed clinically indicated brain MRI/S data from children enrolled in a randomized controlled trial of 24 vs. 72 h of hypothermia following cardiac arrest. Two pediatric radiologists scored conventional MRIs. Lactate and N-acetyl-aspartate (NAA) concentrations (mmol/kg) were determined from spectra acquired from the basal ganglia, thalamus, parietal white matter and parietooccipital gray matter. Mortality and neurological outcomes (favorable = Pediatric Cerebral Performance Category [PCPC] 1, 2, 3 or increase < 2) were assessed at hospital discharge. Non-parametric tests were used to test for associations between MRI/S biomarkers and outcome and randomized group.
23 children with (median [interquartile range]) age of 1.5 (0.3-4.0) years. Ten (44%) had favorable outcome. There were more T2 brain lesions in the lentiform nuclei in children with unfavorable 12 (92%) vs. favorable 3 (33%) outcome, p = 0.007. Increased lactate and decreased NAA concentrations in the parietooccipital gray matter and decreased NAA in the parietal white matter were associated with unfavorable outcome (p's < 0.05). There were no differences for any biomarker by randomized group.
Regional cerebral and metabolic MRI/S biomarkers are predictive of neurological outcomes at hospital discharge in pediatric cardiac arrest and should undergo validation testing in a large sample.
心脏骤停后存活的儿童有很高的神经功能障碍和死亡风险;然而,目前缺乏经过验证的预后生物标志物。我们旨在评估脑磁共振成像(MRI)和磁共振波谱(MRS)作为死亡和残疾预测指标的价值。其次,我们按随机分组评估MRI/MRS情况。
这项单中心研究分析了参与心脏骤停后24小时与72小时低温随机对照试验的儿童的临床指定脑MRI/MRS数据。两名儿科放射科医生对传统MRI进行评分。从基底神经节、丘脑、顶叶白质和顶枕灰质获取的波谱中测定乳酸和N-乙酰天门冬氨酸(NAA)浓度(mmol/kg)。在出院时评估死亡率和神经功能结局(良好=小儿脑功能分类[PCPC]1、2、3或增加<2)。使用非参数检验来检验MRI/MRS生物标志物与结局及随机分组之间的关联。
23名儿童,年龄中位数为1.5岁(四分位间距为0.3 - 4.0岁)。10名(44%)有良好结局。结局不良的儿童豆状核T2脑病变更多,分别为12例(92%)和3例(33%),p = 0.007。顶枕灰质中乳酸增加和NAA浓度降低以及顶叶白质中NAA降低与不良结局相关(p值<0.05)。随机分组后任何生物标志物均无差异。
局部脑和代谢MRI/MRS生物标志物可预测小儿心脏骤停出院时的神经功能结局,应在大样本中进行验证测试。