Neuromodulation Center and Center for Clinical Research Learning, Spaulding Rehabilitation Hospital and Massachusetts General Hospital, Harvard Medical School, 96-13th Street, Charlestown, Boston, MA, USA.
Neuromodulation Center and Center for Clinical Research Learning, Spaulding Rehabilitation Hospital and Massachusetts General Hospital, Harvard Medical School, 96-13th Street, Charlestown, Boston, MA, USA; Universidad San Ignacio de Loyola, Vicerrectorado de Investigación, Unidad de Investigación para la Generación y Síntesis de Evidencias en Salud, Lima, Peru.
Neurophysiol Clin. 2020 Sep;50(4):279-288. doi: 10.1016/j.neucli.2020.06.002. Epub 2020 Jul 9.
Chronic pain is one of the most common and challenging symptoms in fibromyalgia (FM). Currently, self-reported pain is the main criterion used by clinicians assessing patients with pain. However, it is subjective, and multiple factors can affect pain levels. In this study, we investigated the neural correlates of FM pain using conditioned pain modulation (CPM), electroencephalography (EEG), and transcranial magnetic stimulation (TMS).
In this cross-sectional neurophysiological analysis of a randomized, double-blind controlled trial, 36 patients with fibromyalgia were included. We analyzed CPM, EEG variables and TMS measures and their correlation with pain levels as measured by a visual analog scale. Univariate and multivariate linear regression analyses were performed to identify the predictors of pain severity.
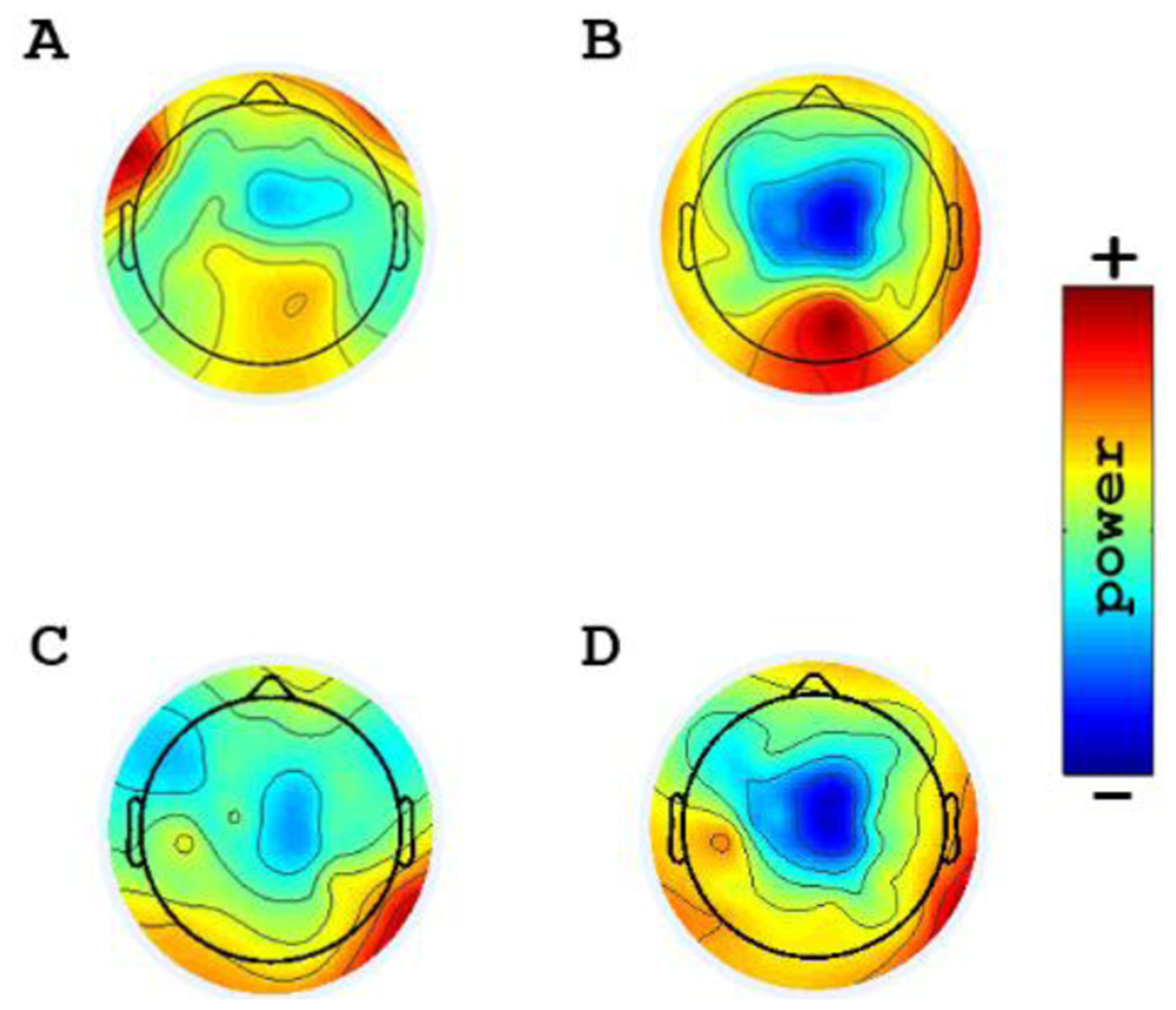
We found: (1) no association between pain levels and CPM; (2) an association between reduced alpha and beta power over the central region in resting-EEG and higher pain levels; (3) an association between smaller event-related desynchronization (ERD) responses in theta and delta bands over the central region and higher pain levels; (4) an association between smaller ERD responses in theta and delta bands and smaller intracortical inhibition and higher intracortical facilitation ratios; (5) an association between smaller ERD responses in delta band and reduced CPM.
Our results do not support CPM as a biomarker for pain intensity in FM. However, our specific EEG findings showing the relationship between pain, CPM and TMS measures suggest that FM leads to a disruption of inhibitory neural modulators and thus support CPM as a likely predictive marker of disrupted pain modulation system. These neurophysiological markers need to be further explored in potential future trials as to find novel targets for the treatment of FM.
慢性疼痛是纤维肌痛(FM)最常见和最具挑战性的症状之一。目前,临床医生评估疼痛患者主要依据自我报告的疼痛。然而,这种方法是主观的,多种因素会影响疼痛程度。在这项研究中,我们使用条件性疼痛调制(CPM)、脑电图(EEG)和经颅磁刺激(TMS)来研究 FM 疼痛的神经相关性。
这是一项随机、双盲对照试验的跨学科神经生理学分析,共纳入 36 名纤维肌痛患者。我们分析了 CPM、脑电图变量和 TMS 测量值及其与视觉模拟量表测量的疼痛程度的相关性。进行了单变量和多变量线性回归分析,以确定疼痛严重程度的预测因素。
我们发现:(1)疼痛程度与 CPM 之间无关联;(2)静息态 EEG 中中央区域的阿尔法和贝塔功率降低与较高的疼痛程度相关;(3)中央区域 theta 和 delta 波段的事件相关去同步(ERD)反应较小与较高的疼痛程度相关;(4)theta 和 delta 波段的 ERD 反应较小与皮质内抑制较小和皮质内易化率较高相关;(5)delta 波段的 ERD 反应较小与 CPM 降低相关。
我们的结果不支持 CPM 作为 FM 疼痛强度的生物标志物。然而,我们的特定脑电图发现表明疼痛、CPM 和 TMS 测量之间的关系表明,FM 导致抑制性神经调节剂的破坏,从而支持 CPM 作为疼痛调节系统破坏的可能预测标志物。这些神经生理学标志物需要在潜在的未来试验中进一步探索,以找到治疗 FM 的新靶点。