Département d'Anesthésie et Réanimation, Hospices Civils de Lyon, Hôpital E. Herriot, Lyon, France.
Service de Réanimation Médicale Infectieuse, APHP, Hôpital Bichat Claude Bernard, Paris, France.
Crit Care. 2020 Jul 14;24(1):434. doi: 10.1186/s13054-020-03114-y.
Improving timeliness of pathogen identification is crucial to allow early adaptation of antibiotic therapy and improve prognosis in patients with pneumonia. We evaluated the relevance of a new syndromic rapid multiplex PCR test (rm-PCR) on respiratory samples to guide empirical antimicrobial therapy in adult patients with community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP), and ventilator-acquired pneumonia (VAP).
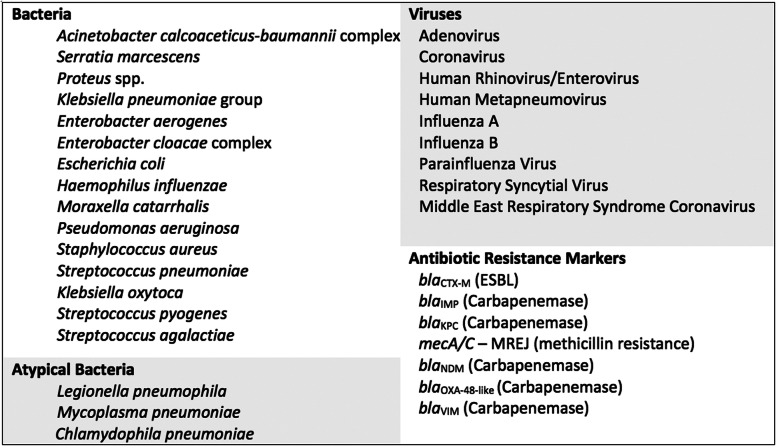
This retrospective multicenter study was conducted in four French university hospitals. Respiratory samples were obtained from patients with clinical and radiological signs of pneumonia and simultaneously tested using conventional microbiological methods and the rm-PCR. A committee composed of an intensivist, a microbiologist, and an infectious diseases specialist retrospectively assessed all medical files and agreed on the most appropriate antimicrobial therapy for each pneumonia episode, according to the results of rm-PCR and blinded to the culture results. The rm-PCR-guided antimicrobial regimen was compared to the empirical treatment routinely administered to the patient in standard care.
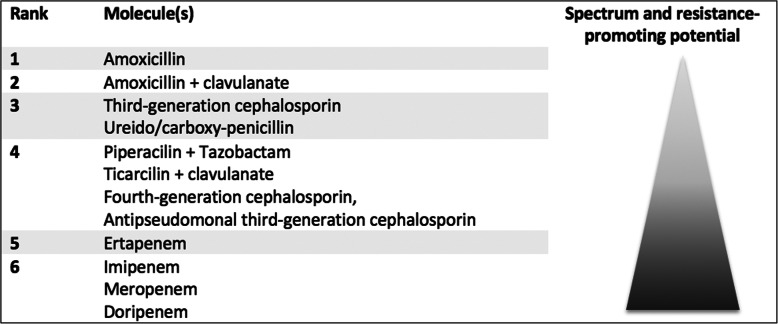
We included 159 pneumonia episodes. Most patients were hospitalized in intensive care units (n = 129, 81%), and episodes were HAP (n = 68, 43%), CAP (n = 54, 34%), and VAP (n = 37, 23%). Conventional culture isolated ≥ 1 microorganism(s) at significant level in 95 (60%) patients. The syndromic rm-PCR detected at least one bacteria in 132 (83%) episodes. Based on the results of the rm-PCR, the multidisciplinary committee proposed a modification of the empirical therapy in 123 (77%) pneumonia episodes. The modification was a de-escalation in 63 (40%), an escalation in 35 (22%), and undetermined in 25 (16%) patients. In microbiologically documented episodes (n = 95), the rm-PCR increased appropriateness of the empirical therapy to 83 (87%), as compared to 73 (77%) in routine care.
Use of a syndromic rm-PCR test has the potential to reduce unnecessary antimicrobial exposure and increase the appropriateness of empirical antibiotic therapy in adult patients with pneumonia.
提高病原体鉴定的及时性对于允许早期适应抗生素治疗并改善肺炎患者的预后至关重要。我们评估了一种新的综合征快速多重 PCR 检测(rm-PCR)在呼吸样本中对社区获得性肺炎(CAP)、医院获得性肺炎(HAP)和呼吸机相关性肺炎(VAP)成年患者经验性抗菌治疗的相关性。
这是一项在法国四所大学医院进行的回顾性多中心研究。从有肺炎临床和影像学表现的患者中获取呼吸道样本,并同时使用常规微生物学方法和 rm-PCR 进行检测。由一名重症监护医生、一名微生物学家和一名传染病专家组成的委员会回顾性评估了所有病历,并根据 rm-PCR 的结果,在不了解培养结果的情况下,就每个肺炎发作的最佳抗菌治疗方案达成一致意见。rm-PCR 指导的抗菌方案与标准护理中常规给予患者的经验性治疗进行了比较。
我们纳入了 159 例肺炎发作。大多数患者在重症监护病房(n=129,81%)住院,发作类型为 HAP(n=68,43%)、CAP(n=54,34%)和 VAP(n=37,23%)。常规培养在 95 例(60%)患者中分离出≥1 种有意义的微生物。综合征 rm-PCR 在 132 例(83%)发作中至少检测到 1 种细菌。根据 rm-PCR 的结果,多学科委员会建议修改 123 例(77%)肺炎发作的经验性治疗方案。修改方案包括 63 例(40%)降级、35 例(22%)升级和 25 例(16%)未确定。在微生物学确诊的病例(n=95)中,rm-PCR 将经验性治疗的适当性提高到 83%(87%),而常规治疗为 73%(77%)。
使用综合征 rm-PCR 检测有可能减少不必要的抗菌药物暴露,并提高成年肺炎患者经验性抗生素治疗的适当性。