Bertelsen Litten, Vejlstrup Niels, Andreasen Laura, Olesen Morten Salling, Svendsen Jesper Hastrup
Department of Cardiology, Centre for Cardiac, Vascular, Pulmonary and Infectious Diseases, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark
Department of Cardiology, Centre for Cardiac, Vascular, Pulmonary and Infectious Diseases, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark.
Open Heart. 2020 Jul;7(2). doi: 10.1136/openhrt-2020-001323.
Cardiac MRI is quickly emerging as the gold standard for assessment of mitral regurgitation, most commonly with the indirect method subtracting forward flow in aorta from volumetric segmentation of the left ventricle. We aimed to investigate how aortic flow measurements with increasing distance from the aortic valve affect calculated mitral regurgitations and whether measurements were influenced by breath-hold regimen.
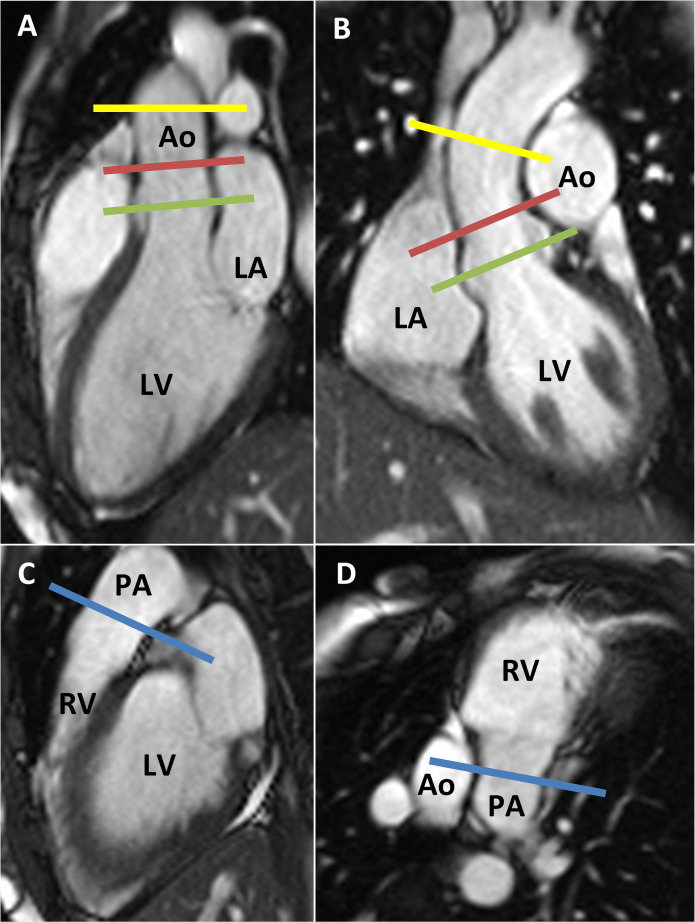
Free-breathing and breath-hold phase contrast flows were measured in aorta at valve level, sinotubular (ST) junction, mid-ascending aorta and in the pulmonary trunk. Flow measurements were pairwise compared, and subsequently, after exclusion of patients with visible mitral and tricuspid regurgitations for left-sided and right-sided comparisons, respectively, flow-measured stroke volumes were compared with ventricular volumetric segmentations.
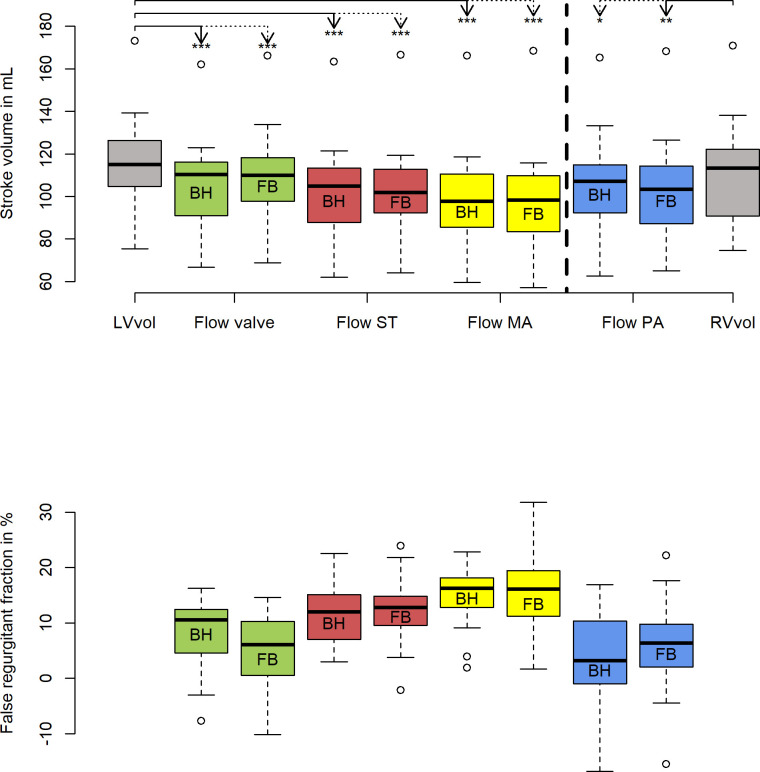
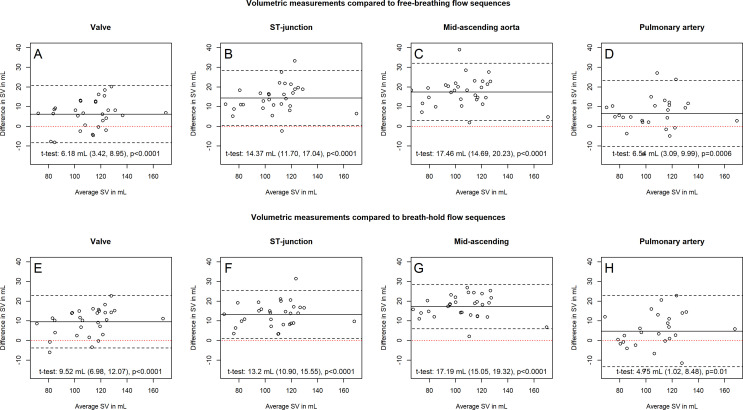
Thirty-nine participants without arrhythmias or structural abnormalities of the large vessels were included. Stroke volumes measured with free-breathing and breath-hold flow decreased equally with increasing distance to the aortic valves (breath-hold flow: aortic valve 105.6±20.8 mL, ST junction 101.5±20.7 mL, mid-ascending aorta 98.1±21.5 mL). After exclusion of atrioventricular regurgitations, stroke volumes determined by volumetric measurements were higher compared with values determined by flow measurements, corresponding to 'false' atrioventricular regurgitations of 8.0%±5.8% with flow measured at valve level, 11.6%±5.2% at the ST junction and 15.3%±5.0% at the mid-ascending aorta.
Stroke volumes determined by flow decrease throughout the proximal aorta and are systematically lower than volumetrically measured stroke volumes. The indirect method systematically overestimates mitral regurgitations, especially with increasing distance from the aortic valves.
心脏磁共振成像正迅速成为评估二尖瓣反流的金标准,最常用的间接方法是通过左心室容积分割减去主动脉内的前向血流。我们旨在研究距主动脉瓣距离增加时主动脉血流测量如何影响计算出的二尖瓣反流,以及测量是否受屏气方案的影响。
在主动脉瓣水平、窦管(ST)交界处、升主动脉中部和肺动脉主干处,对自由呼吸和屏气状态下的相位对比血流进行测量。对血流测量值进行两两比较,随后,在分别排除左侧和右侧可见二尖瓣和三尖瓣反流的患者后,将血流测量的每搏输出量与心室容积分割结果进行比较。
纳入39名无心律失常或大血管结构异常的参与者。自由呼吸和屏气血流测量的每搏输出量均随距主动脉瓣距离增加而同等程度下降(屏气血流:主动脉瓣处105.6±20.8 mL,ST交界处101.5±20.7 mL,升主动脉中部98.1±21.5 mL)。排除房室反流后,容积测量确定的每搏输出量高于血流测量值,对应于在瓣膜水平血流测量时“假性”房室反流为8.0%±5.8%,在ST交界处为11.6%±5.2%,在升主动脉中部为15.3%±5.0%。
通过血流测定的每搏输出量在整个近端主动脉中均下降,且系统性低于容积测量的每搏输出量。间接方法系统性高估二尖瓣反流,尤其是距主动脉瓣距离增加时。