Smith Bradford J, Roy Gregory S, Cleveland Alyx, Mattson Courtney, Okamura Kayo, Charlebois Chantel M, Hamlington Katharine L, Novotny Michael V, Knudsen Lars, Ochs Matthias, Hite R Duncan, Bates Jason H T
Department of Bioengineering, College of Engineering, Design & Computing, University of Colorado Denver | Anschutz Medical Campus, Aurora, CO, United States.
Department of Pediatric Pulmonary and Sleep Medicine, School of Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO, United States.
Front Physiol. 2020 Jun 30;11:660. doi: 10.3389/fphys.2020.00660. eCollection 2020.
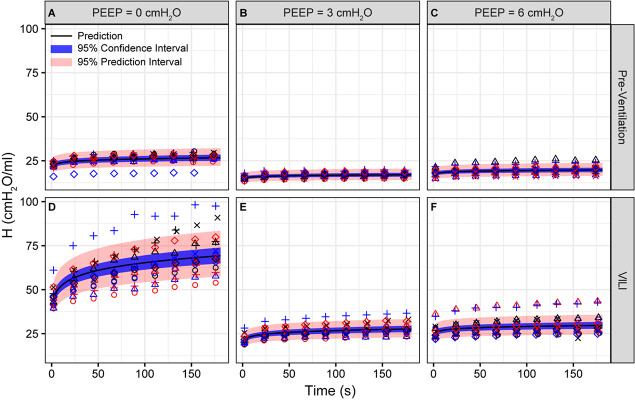
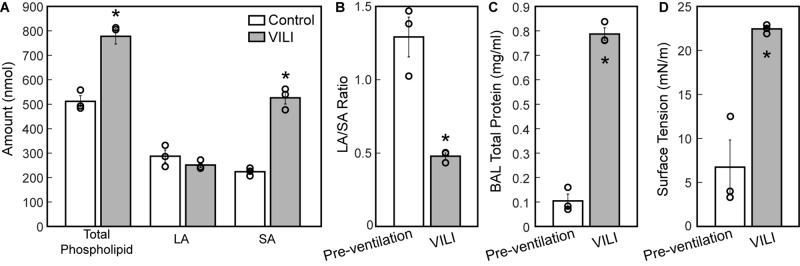
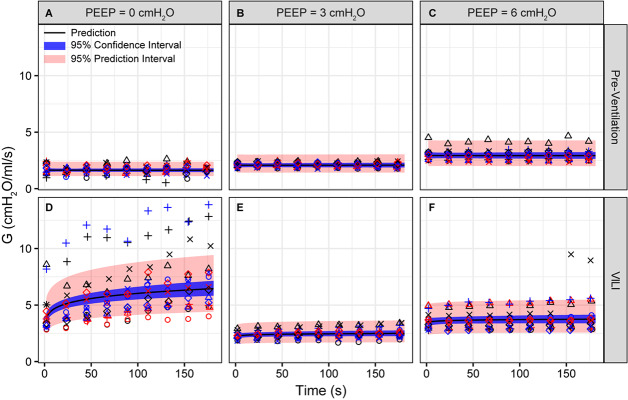
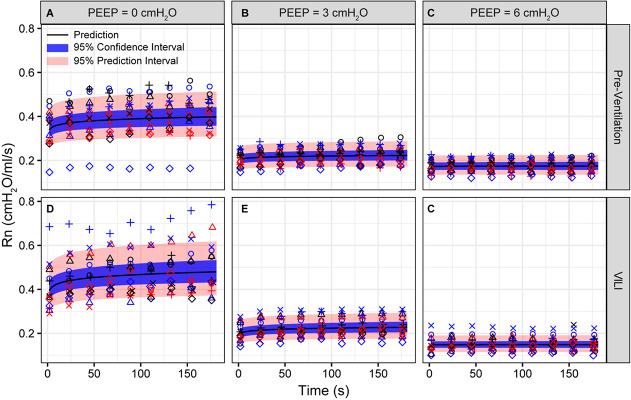
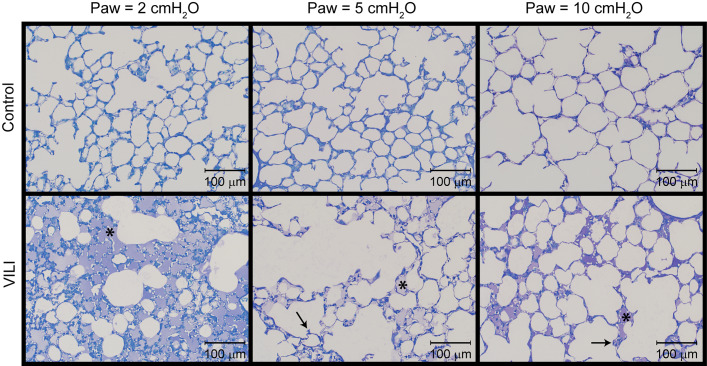
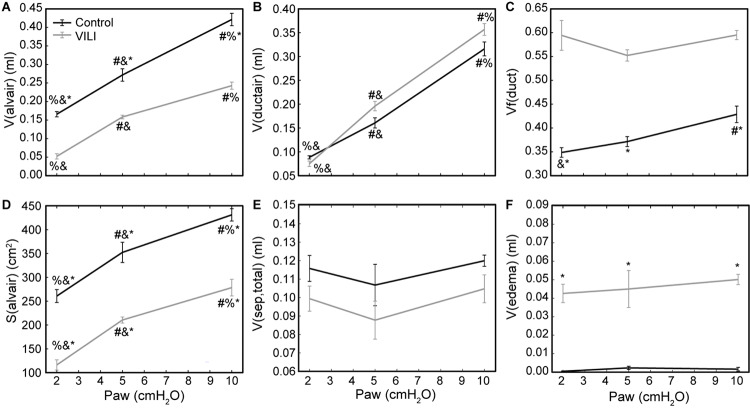
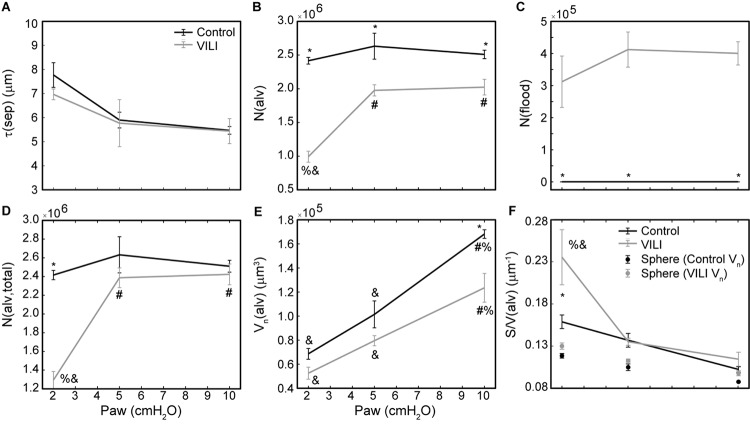
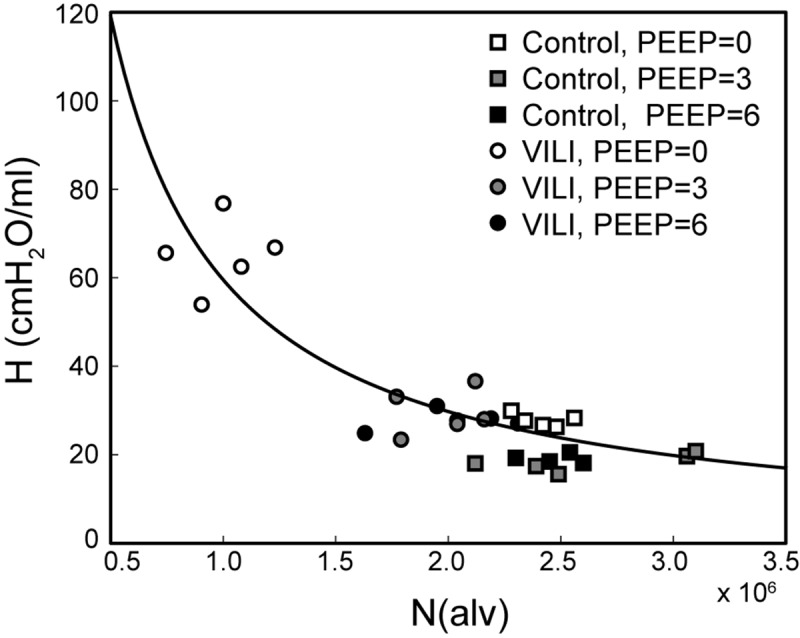
Mechanical ventilation is an essential lifesaving therapy in acute respiratory distress syndrome (ARDS) that may cause ventilator-induced lung injury (VILI) through a positive feedback between altered alveolar mechanics, edema, surfactant inactivation, and injury. Although the biophysical forces that cause VILI are well documented, a knowledge gap remains in the quantitative link between altered parenchymal structure (namely alveolar derecruitment and flooding), pulmonary function, and VILI. This information is essential to developing diagnostic criteria and ventilation strategies to reduce VILI and improve ARDS survival. To address this unmet need, we mechanically ventilated mice to cause VILI. Lung structure was measured at three air inflation pressures using design-based stereology, and the mechanical function of the pulmonary system was measured with the forced oscillation technique. Assessment of the pulmonary surfactant included total surfactant, distribution of phospholipid aggregates, and surface tension lowering activity. VILI-induced changes in the surfactant included reduced surface tension lowering activity in the typically functional fraction of large phospholipid aggregates and a significant increase in the pool of surface-inactive small phospholipid aggregates. The dominant alterations in lung structure at low airway pressures were alveolar collapse and flooding. At higher airway pressures, alveolar collapse was mitigated and the flooded alveoli remained filled with proteinaceous edema. The loss of ventilated alveoli resulted in decreased alveolar gas volume and gas-exchange surface area. These data characterize three alveolar phenotypes in murine VILI: flooded and non-recruitable alveoli, unstable alveoli that derecruit at airway pressures below 5 cmHO, and alveoli with relatively normal structure and function. The fraction of alveoli with each phenotype is reflected in the proportional changes in pulmonary system elastance at positive end expiratory pressures of 0, 3, and 6 cmHO.
机械通气是急性呼吸窘迫综合征(ARDS)中一项至关重要的挽救生命的治疗方法,但它可能通过肺泡力学改变、水肿、表面活性剂失活和损伤之间的正反馈作用导致呼吸机诱导的肺损伤(VILI)。尽管导致VILI的生物物理力已得到充分记录,但在实质结构改变(即肺泡萎陷和充盈)、肺功能与VILI之间的定量联系方面仍存在知识空白。这些信息对于制定诊断标准和通气策略以减少VILI并提高ARDS患者生存率至关重要。为满足这一未被满足的需求,我们对小鼠进行机械通气以诱导VILI。使用基于设计的体视学方法在三种充气压力下测量肺结构,并采用强迫振荡技术测量肺系统的机械功能。对肺表面活性剂的评估包括总表面活性剂、磷脂聚集体的分布以及表面张力降低活性。VILI诱导的表面活性剂变化包括大磷脂聚集体的典型功能部分中表面张力降低活性降低,以及表面无活性的小磷脂聚集体池显著增加。低气道压力下肺结构的主要改变是肺泡萎陷和充盈。在较高气道压力下,肺泡萎陷得到缓解,充盈的肺泡仍充满蛋白质性水肿。通气肺泡的减少导致肺泡气体容积和气体交换表面积降低。这些数据描述了小鼠VILI中的三种肺泡表型:充盈且不可复张的肺泡、在气道压力低于5 cmH₂O时萎陷的不稳定肺泡,以及结构和功能相对正常的肺泡。每种表型的肺泡比例反映在呼气末正压为0、3和6 cmH₂O时肺系统弹性的比例变化中。