Duke Cancer Institute, Duke University Medical Center, Durham, North Carolina, USA.
Weill Cornell Medicine, New York, New York, USA.
Oncologist. 2020 Nov;25(11):e1655-e1662. doi: 10.1634/theoncologist.2020-0679. Epub 2020 Aug 20.
The results from the liposarcoma cohort of SARC024 confirm previously published data and do not support the routine use of regorafenib in this patient population. Continued exploration of novel therapies, including combination approaches, is warranted for a patient population in whom limited treatment options exist.
Regorafenib is a multitargeted kinase inhibitor with a kinase profile overlapping, but distinct from, pazopanib, an agent approved for recurrent and metastatic non-gastrointestinal stromal tumor (GIST), non-adipocytic soft tissue sarcoma. We conducted a randomized, phase II study of regorafenib versus placebo in refractory liposarcoma patients.
Patients with advanced or metastatic, treatment-refractory liposarcoma were randomized 1:1 to receive regorafenib 160 mg or placebo once daily (3 weeks on, 1 week off). Patients with well-differentiated liposarcoma only were excluded. Crossover for placebo was allowed upon progression. The primary endpoint was progression-free survival (PFS), according to RECIST version 1.1.
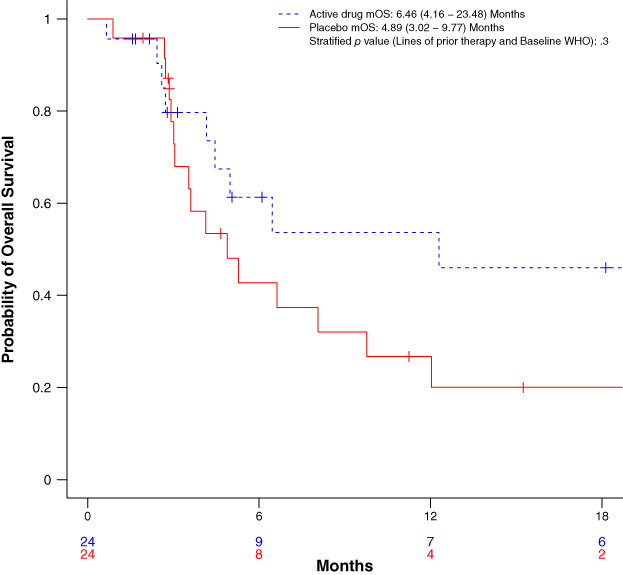
Forty-eight subjects with liposarcoma (34 dedifferentiated, 12 myxoid/round cell, 2 pleomorphic) were enrolled. Median PFS was 1.87 (95% confidence interval [CI], 0.92-3.67) months for regorafenib versus 2.07 (95% CI, 1.64-3.44) months for placebo; stratified hazard ratio [HR], 0.85 (95% CI, 0.46, 1.58), p = .62. No responses were seen on regorafenib. One PR was observed on placebo. Median overall survival was 6.46 (95% CI, 4.16-23.48) months for regorafenib and 4.89 (95% CI, 3.02-9.77) months for placebo, stratified HR, 0.66 (95% CI, 0.31-1.40), p = .28). Treatment-related adverse events were similar to the known safety profile of regorafenib.
Regorafenib did not appear to improve PFS in treatment-refractory liposarcoma. No new significant safety signals were observed.
SARC024 脂肪肉瘤队列的结果证实了先前发表的数据,并不支持常规使用regorafenib 治疗此类患者。对于治疗选择有限的患者群体,需要继续探索新的治疗方法,包括联合治疗方法。
regorafenib 是一种多靶点激酶抑制剂,其激酶谱与批准用于复发性和转移性非胃肠道间质瘤(GIST)、非脂肪性软组织肉瘤的 pazopanib 重叠但又不同。我们进行了一项随机、II 期研究,比较了 regorafenib 与安慰剂在难治性脂肪肉瘤患者中的疗效。
患有晚期或转移性、治疗耐药性脂肪肉瘤的患者按 1:1 随机接受regorafenib 160mg 或安慰剂,每日一次(连续 3 周,1 周停药)。仅排除分化良好的脂肪肉瘤患者。安慰剂组在进展后允许交叉使用。主要终点是根据 RECIST 版本 1.1 评估的无进展生存期(PFS)。
共纳入 48 例脂肪肉瘤患者(34 例去分化型、12 例黏液样/圆形细胞型、2 例多形性)。regorafenib 组的中位 PFS 为 1.87 个月(95%CI,0.92-3.67),安慰剂组为 2.07 个月(95%CI,1.64-3.44);分层风险比[HR]为 0.85(95%CI,0.46-1.58),p =.62。regorafenib 组未观察到缓解。安慰剂组观察到 1 例部分缓解。regorafenib 组的中位总生存期为 6.46 个月(95%CI,4.16-23.48),安慰剂组为 4.89 个月(95%CI,3.02-9.77),分层 HR 为 0.66(95%CI,0.31-1.40),p =.28)。治疗相关不良事件与 regorafenib 的已知安全性特征相似。
regorafenib 似乎并未改善治疗耐药性脂肪肉瘤患者的 PFS。未观察到新的显著安全性信号。