MMWR Recomm Rep. 2020 Jul 24;69(6):1-8. doi: 10.15585/mmwr.rr6906a1.
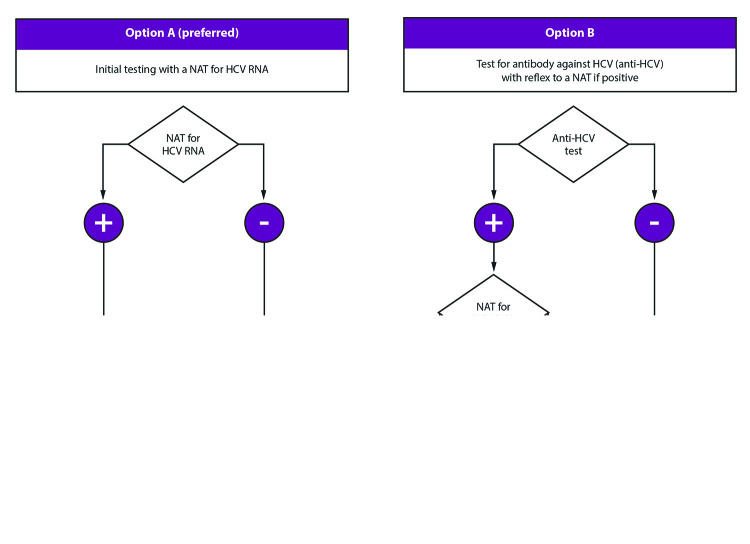
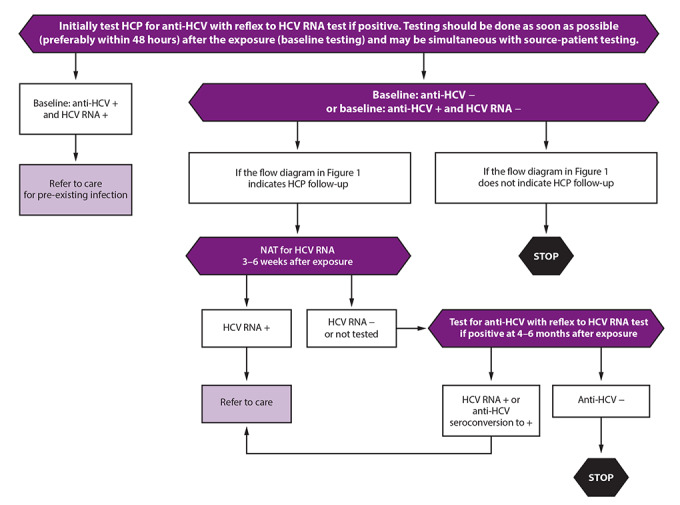
Exposure to hepatitis viruses is a recognized occupational risk for health care personnel (HCP). This report establishes new CDC guidance that includes recommendations for a testing algorithm and clinical management for HCP with potential occupational exposure to hepatitis C virus (HCV). Baseline testing of the source patient and HCP should be performed as soon as possible (preferably within 48 hours) after the exposure. A source patient refers to any person receiving health care services whose blood or other potentially infectious material is the source of the HCP's exposure. Two options are recommended for testing the source patient. The first option is to test the source patient with a nucleic acid test (NAT) for HCV RNA. This option is preferred, particularly if the source patient is known or suspected to have recent behaviors that increase risk for HCV acquisition (e.g., injection drug use within the previous 4 months) or if risk cannot be reliably assessed. The second option is to test the source patient for antibodies to hepatitis C virus (anti-HCV), then if positive, test for HCV RNA. For HCP, baseline testing for anti-HCV with reflex to a NAT for HCV RNA if positive should be conducted as soon as possible (preferably within 48 hours) after the exposure and may be simultaneous with source-patient testing. If follow-up testing is recommended based on the source patient's status (e.g., HCV RNA positive or anti-HCV positive with unavailable HCV RNA or if the HCV infection status is unknown), HCP should be tested with a NAT for HCV RNA at 3-6 weeks postexposure. If HCV RNA is negative at 3-6 weeks postexposure, a final test for anti-HCV at 4-6 months postexposure is recommended. A source patient or HCP found to be positive for HCV RNA should be referred to care. Postexposure prophylaxis of hepatitis C is not recommended for HCP who have occupational exposure to blood and other body fluids. This guidance was developed based on expert opinion (CDC. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. MMWR Recommend Rep 2001;50[No. RR-11]; Supplementary Figure, https://stacks.cdc.gov/view/cdc/90288) and reflects updated guidance from professional organizations that recommend treatment for acute HCV infection. Health care providers can use this guidance to update their procedures for postexposure testing and clinical management of HCP potentially exposed to hepatitis C virus.
接触肝炎病毒是卫生保健人员(HCP)公认的职业风险。本报告制定了新的 CDC 指南,其中包括对可能发生职业性接触丙型肝炎病毒(HCV)的 HCP 进行检测算法和临床管理的建议。应尽快(最好在暴露后 48 小时内)对源患者和 HCP 进行基线检测。源患者是指接受医疗服务的任何人,其血液或其他潜在传染性物质是 HCP 暴露的来源。建议对源患者进行两种检测选择。第一种选择是使用 HCV RNA 核酸检测(NAT)对源患者进行检测。如果源患者最近有增加 HCV 感染风险的行为(例如,在过去 4 个月内注射吸毒)或无法可靠评估风险,则首选此选项。第二种选择是对源患者进行抗丙型肝炎病毒(抗-HCV)抗体检测,如果阳性,则检测 HCV RNA。对于 HCP,应尽快(最好在暴露后 48 小时内)进行抗-HCV 基线检测,如果阳性,应进行 HCV RNA 的 NAT 检测。如果根据源患者的情况建议进行后续检测(例如,HCV RNA 阳性或抗-HCV 阳性但 HCV RNA 不可用,或 HCV 感染状况未知),应在暴露后 3-6 周对 HCP 进行 HCV RNA 的 NAT 检测。如果 HCV RNA 在暴露后 3-6 周为阴性,则建议在暴露后 4-6 个月进行最后一次抗-HCV 检测。如果源患者或 HCP 检测到 HCV RNA 阳性,应转介接受治疗。不建议对发生血液和其他体液职业性暴露的 HCP 进行丙型肝炎暴露后预防。本指南是基于专家意见(CDC. 更新的美国公共卫生服务指南,用于管理乙型肝炎病毒、丙型肝炎病毒和 HIV 的职业暴露以及推荐的暴露后预防措施。MMWR 推荐报告 2001;50[No. RR-11];补充图,https://stacks.cdc.gov/view/cdc/90288)制定的,反映了专业组织更新的建议,即对急性 HCV 感染进行治疗。卫生保健提供者可以使用本指南更新他们对可能接触丙型肝炎病毒的 HCP 进行暴露后检测和临床管理的程序。