Evidence Synthesis, Modeling & Communication Evidera Inc, Waltham, MA, USA.
Amgen Inc, Global Health Economics, Thousand Oaks, CA, USA.
Health Qual Life Outcomes. 2020 Jul 27;18(1):251. doi: 10.1186/s12955-020-01407-y.
Identify the most recent utility value estimates for cardiovascular disease (CVD) via systematic literature review (SLR) and explore trends in utility elicitation methods in the last 6 years.
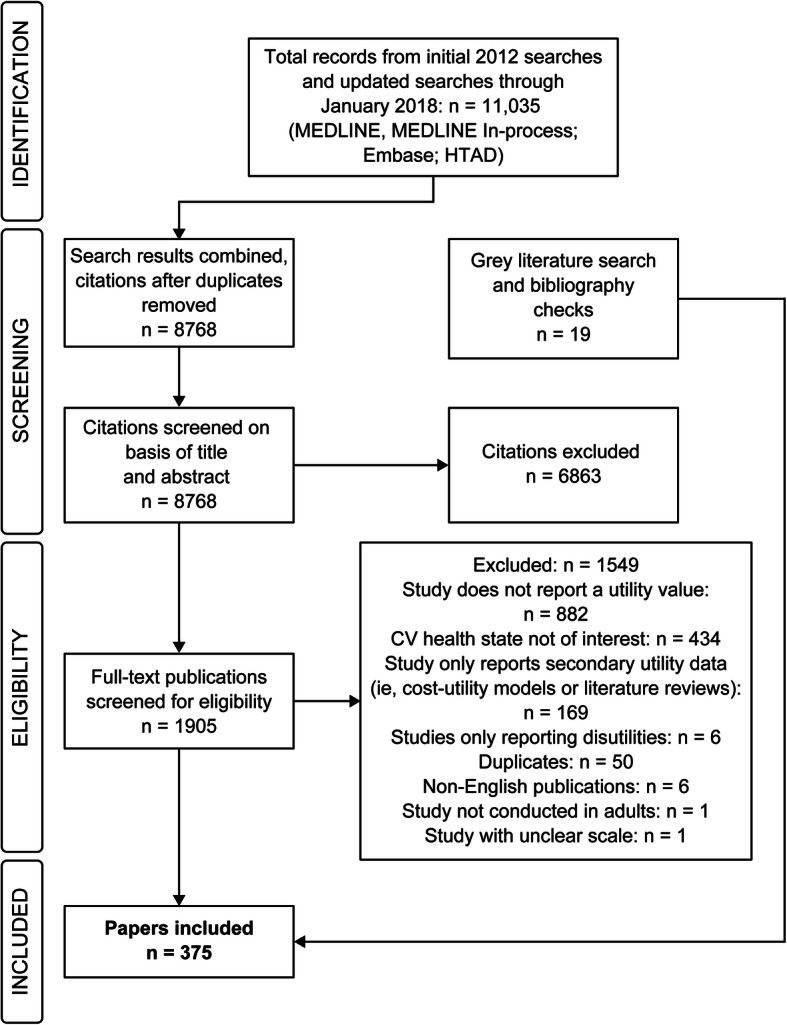
This SLR was updated on January 25, 2018, and identified studies reporting utilities for myocardial infarction (MI), stroke, angina, peripheral artery disease (PAD), and any-cause revascularization by searching Embase, PubMed, Health Technology Assessment Database, and grey literature.
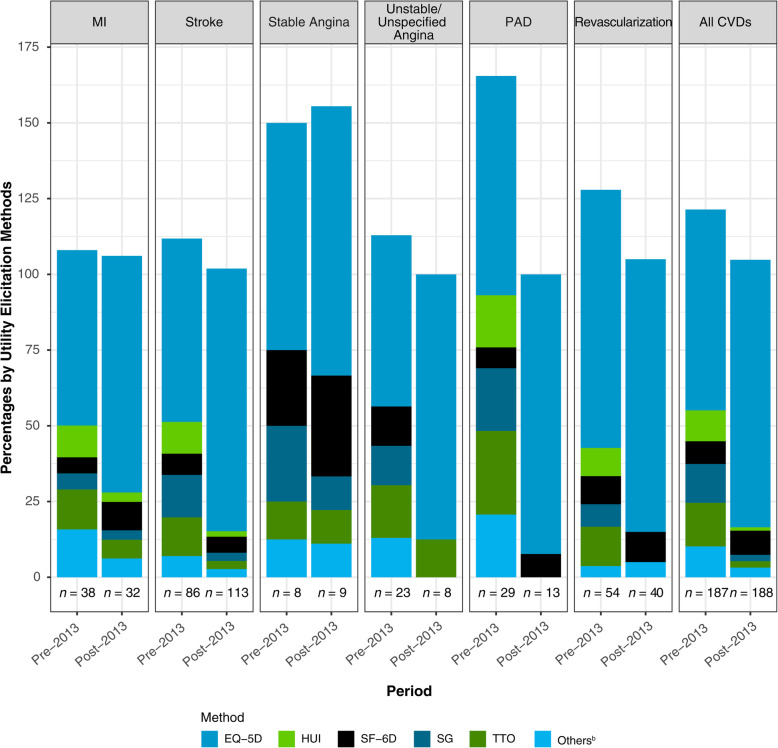
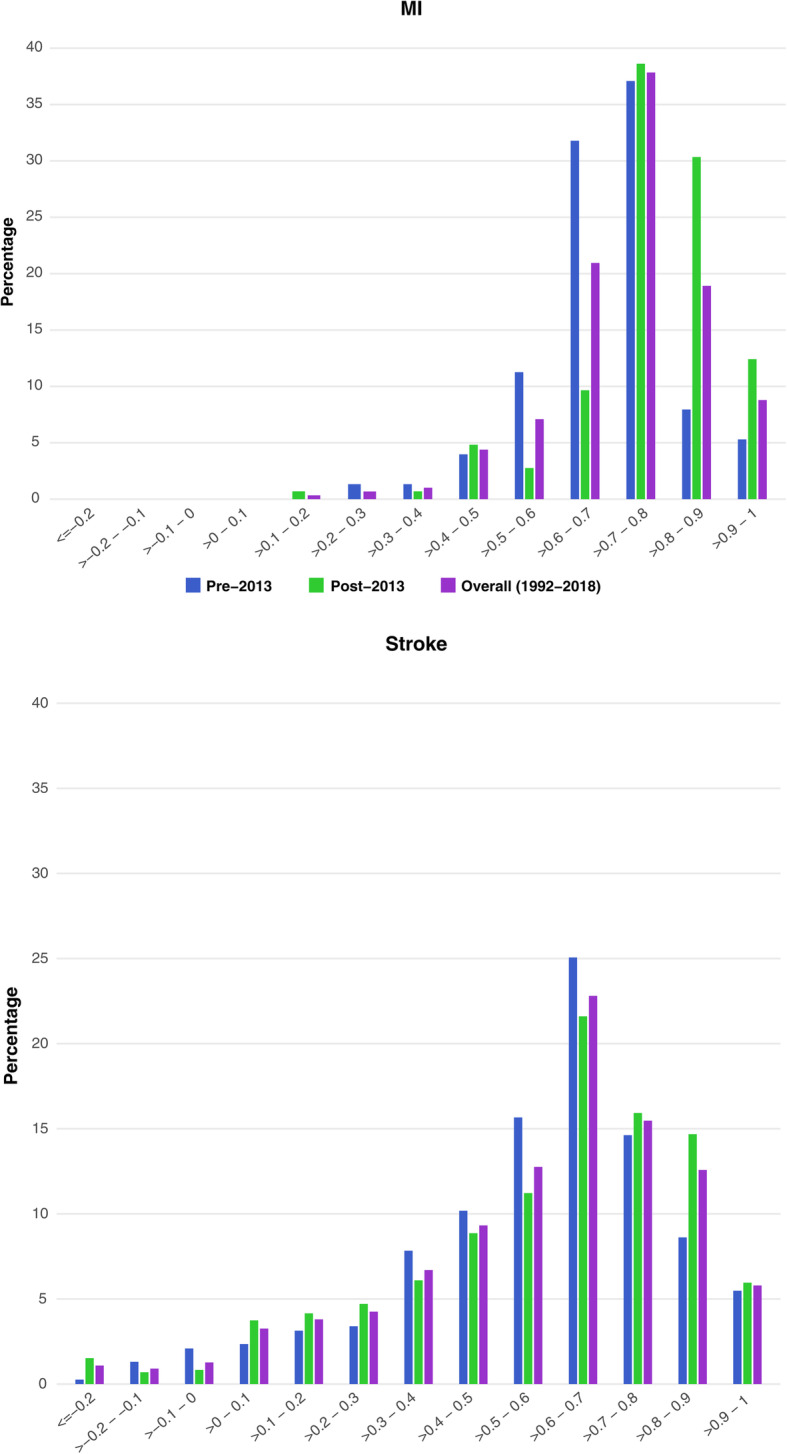
A total of 375 studies reported CVD utilities (pre-2013 vs post-2013: MI, 38 vs 32; stroke, 86 vs 113; stable angina, 8 vs 9; undefined/unstable angina, 23 vs 8; PAD, 29 vs 13; revascularization, 54 vs 40). Median average utilities for MI, stroke, and revascularization increased over time (pre-2013 vs post-2013: MI, 0.71 vs 0.79; stroke, 0.63 vs 0.64; revascularization, 0.76 vs 0.81); angina and PAD showed a decrease in median values over time (stable angina, 0.83 vs 0.72; undefined/unstable angina, 0.70 vs 0.69; PAD, 0.76 vs 0.71). The proportion of utility estimates from trials increased across health states (pre-2013 vs post-2013: 22.5% vs 37.2%), as did the proportion of trials using the EuroQol Five Dimensions Questionnaire (EQ-5D; pre-2013 vs post-2013: 73.8% vs 91.4%). Use of methods such as the standard gamble, time trade-off, and Health Utilities Index has declined.
Health state utilities for cardiovascular health states have changed in the last 6 years, likely due to changes in the types of studies conducted, the patient populations evaluated, and possibly changing utility elicitation methods. The EQ-5D has been used more frequently.
通过系统文献回顾(SLR)确定最近心血管疾病(CVD)的实用价值评估,并探讨过去 6 年中实用评估方法的趋势。
本 SLR 于 2018 年 1 月 25 日进行了更新,通过搜索 Embase、PubMed、卫生技术评估数据库和灰色文献,确定了报告心肌梗死(MI)、中风、心绞痛、外周动脉疾病(PAD)和任何原因血运重建的效用的研究。
共有 375 项研究报告了 CVD 效用(2013 年前 vs 2013 年后:MI,38 项 vs 32 项;中风,86 项 vs 113 项;稳定型心绞痛,8 项 vs 9 项;未定义/不稳定型心绞痛,23 项 vs 8 项;PAD,29 项 vs 13 项;血运重建,54 项 vs 40 项)。MI、中风和血运重建的平均效用中位数随时间推移而增加(2013 年前 vs 2013 年后:MI,0.71 vs 0.79;中风,0.63 vs 0.64;血运重建,0.76 vs 0.81);心绞痛和 PAD 的中位数值随时间推移而降低(稳定型心绞痛,0.83 vs 0.72;未定义/不稳定型心绞痛,0.70 vs 0.69;PAD,0.76 vs 0.71)。健康状态的效用评估比例在各个健康状态下均有所增加(2013 年前 vs 2013 年后:22.5% vs 37.2%),同时使用欧洲五维健康量表(EQ-5D;2013 年前 vs 2013 年后:73.8% vs 91.4%)的比例也有所增加。标准博弈、时间权衡和健康效用指数等方法的使用有所减少。
在过去的 6 年中,心血管健康状况的健康状态效用发生了变化,这可能是由于所进行的研究类型、评估的患者人群以及可能发生的效用评估方法的变化所致。EQ-5D 的使用频率更高。