Division of Colorectal Surgery, Department of Surgery, LAC+USC, Los Angeles, CA, USA.
, 1441 Eastlake Ave, Suite NTT-7418, Los Angeles, CA, 90033-4612, USA.
J Gastrointest Surg. 2021 Jan;25(1):260-268. doi: 10.1007/s11605-020-04722-3. Epub 2020 Jul 27.
All elective surgeries have been postponed at our institution starting 3/16/20 due to the COVID-19 pandemic. We assessed changes in hospital resource utilization and estimated the future backlog of cases in the colorectal surgery division of a large safety-net hospital.
Patients undergoing colorectal procedures from 3/16/20 to 4/23/20 (COVID) were compared with those from January through June 2018 (historical). Resource utilization rates were calculated by weekly case volumes and hospital stay in each group. A future catch up timeframe and new wait times from scheduling to surgery dates were calculated.
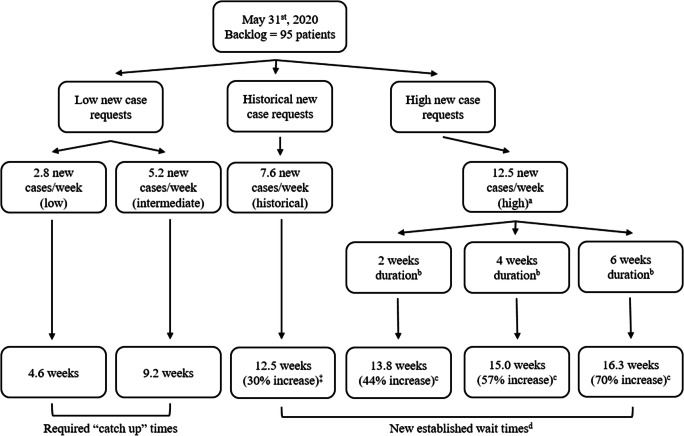
The COVID and historical groups included 13 and 239 patients, respectively. The COVID group showed a 74% relative decrease in weekly surgical case rates (9.2 to 2.4 patients per week). Both groups had similar lengths of stay. The COVID group had a longer average ICU stay (1.4 ± 2.5 days vs. 0.4 ± 1.2 days, P = 0.016) and a 132% increase in ICU resource utilization. Overall, the COVID group had a 48% relative decrease in hospital resource utilization, owing to reduced volume but higher acuity. If the surgery numbers returns to pre-COVID volumes, the calculated "catch up" times range from 4.6 weeks to 9.2 weeks. Wait times for new cases may increase by 70% compared with pre-COVID levels.
Cancelling elective colorectal surgeries results in a decrease in overall but increase in ICU-specific resource utilization. Though necessary, cancellations result in an increasing backlog of cases that poses significant future logistical and clinical challenges in an already overburdened safety-net hospital. Effective triage systems will be critical to prioritize this backlog.
由于 COVID-19 大流行,我们机构从 3 月 16 日开始暂停所有择期手术。我们评估了医院资源利用情况的变化,并估计了一家大型保障医院结直肠外科部门未来积压病例的情况。
将 3 月 16 日至 4 月 23 日(COVID 期间)接受结直肠手术的患者与 2018 年 1 月至 6 月(历史)期间的患者进行比较。通过每组每周的病例量和住院时间计算资源利用率。计算了未来追赶时间表和从安排手术日期到手术日期的新等待时间。
COVID 组和历史组分别包括 13 例和 239 例患者。COVID 组每周手术例数相对减少 74%(9.2 例/周至 2.4 例/周)。两组的住院时间相似。COVID 组 ICU 平均停留时间较长(1.4 ± 2.5 天 vs. 0.4 ± 1.2 天,P = 0.016),ICU 资源利用率增加 132%。总体而言,COVID 组由于手术量减少但病情加重,医院资源利用率相对减少 48%。如果手术数量恢复到 COVID 前的水平,计算出的“追赶”时间范围为 4.6 周至 9.2 周。与 COVID 前相比,新病例的等待时间可能增加 70%。
取消择期结直肠手术导致总体资源利用率下降,但 ICU 特定资源利用率增加。尽管有必要,但取消手术会导致积压病例增加,这对已经负担过重的保障医院来说,未来会带来重大的后勤和临床挑战。有效的分诊系统对于优先处理这一积压病例至关重要。