Stanley Jemima C, Deng Hong
Pathology, Zhejiang University School of Medicine, Hangzhou, CHN.
Cureus. 2020 Jun 23;12(6):e8789. doi: 10.7759/cureus.8789.
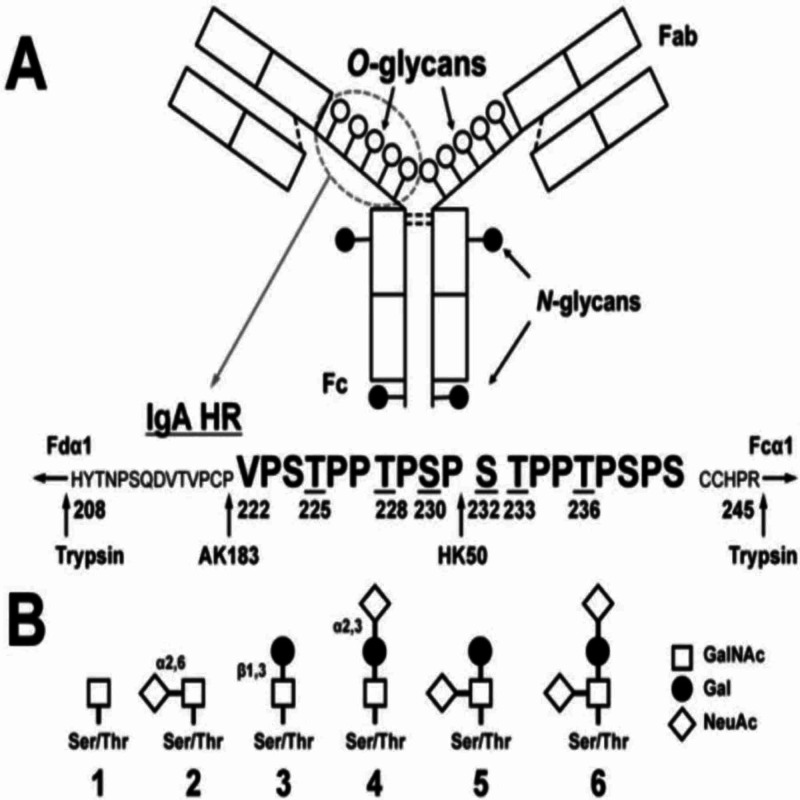
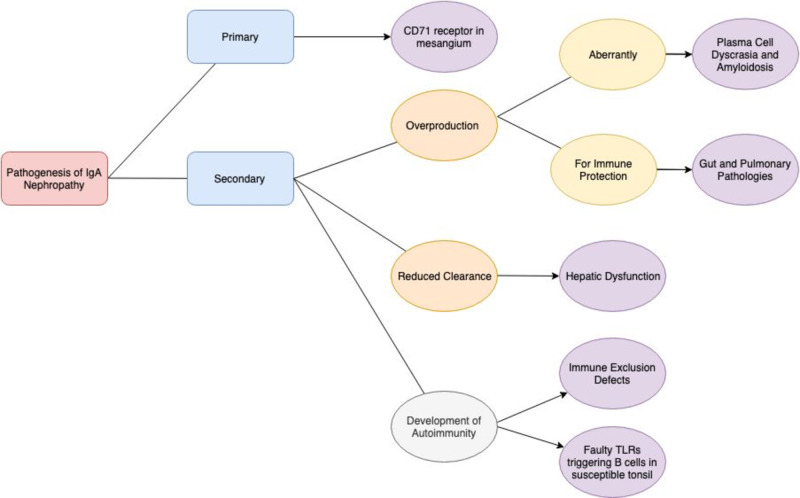
The understanding of the pathogenesis of any disease is the key to effective and specific treatment of the disease. immunoglobulin A (IgA) nephropathy is an autoimmune disease of the kidney. Oxford MEST classification is commonly used to stratify patients according to the severity of the disease. Patients with IgA nephropathy seem to produce anti-GalNAc antibodies against a particularly defective IgA1. This immune complex deposits in the kidneys, leading to a type 3 hypersensitivity reaction which ultimately damages the kidneys. People of a certain genetic background and who experience upregulation of certain defective receptors seem to develop primary IgA nephropathy. Secondary IgA nephropathy could be due to dysbiosis of the microbiota in the gut, compromised gut immunity or other gut pathologies, pulmonary function abnormalities, or amyloidosis. Overproduction of IgA due to plasma cell dyscrasia or reduced clearance of IgA due to liver abnormalities could also be potential causes. Genes that predispose individuals to IgA nephropathy and intestinal abnormalities, such as Celiac disease, seem to overlap and these people tend to have a poorer prognosis and need to be placed on more intensive treatment regimens. IgA Vasculitis seems to be a systemic form of IgA nephropathy, whereby IgA deposits systemically and leads to multiple disease manifestations. Patients in high-risk groups could also be prophylactically screened for the disease and closely monitored by immunohistochemical methods such as an enzyme-linked immunosorbent assay (ELISA) or identified by genetic testing. Currently, the major treatment regimens involve supportive therapy or immunosuppressive therapy which has major side effects. More specific treatment methods such as monoclonal antibodies, immunoglobulin replacement therapy, or low-antigen-content diet could also be looked into as potential treatment options. Stem cell replacement, by way of bone marrow transplant and tonsillectomy, has been suggested as a treatment option in patients with indications.
对任何疾病发病机制的理解是有效且特异性治疗该疾病的关键。免疫球蛋白A(IgA)肾病是一种肾脏自身免疫性疾病。牛津MEST分类法通常用于根据疾病严重程度对患者进行分层。IgA肾病患者似乎会产生针对一种特别有缺陷的IgA1的抗GalNAc抗体。这种免疫复合物沉积在肾脏中,导致Ⅲ型超敏反应,最终损害肾脏。具有特定遗传背景且某些缺陷受体上调的人似乎会患上原发性IgA肾病。继发性IgA肾病可能是由于肠道微生物群失调、肠道免疫功能受损或其他肠道病变、肺功能异常或淀粉样变性。浆细胞发育异常导致IgA产生过多或肝脏异常导致IgA清除减少也可能是潜在原因。使个体易患IgA肾病和肠道异常(如乳糜泻)的基因似乎存在重叠,这些人往往预后较差,需要采用更强化的治疗方案。IgA血管炎似乎是IgA肾病的一种全身性形式,即IgA全身性沉积并导致多种疾病表现。高危人群的患者也可通过酶联免疫吸附测定(ELISA)等免疫组织化学方法进行疾病的预防性筛查和密切监测,或通过基因检测进行识别。目前,主要的治疗方案包括支持性治疗或有重大副作用的免疫抑制治疗。单克隆抗体、免疫球蛋白替代疗法或低抗原含量饮食等更具特异性的治疗方法也可作为潜在的治疗选择进行研究。对于有适应证的患者,已建议通过骨髓移植和扁桃体切除术进行干细胞替代治疗。