Exercise Physiology Research Group, Department of Movement Sciences, KU Leuven, Leuven, BELGIUM.
Med Sci Sports Exerc. 2021 Feb 1;53(2):431-441. doi: 10.1249/MSS.0000000000002467.
We recently reported that oral ketone ester (KE) intake before and during the initial 30 min of a 3 h 15 min simulated cycling race (RACE) transiently decreased blood pH and bicarbonate without affecting maximal performance in the final quarter of the event. We hypothesized that acid-base disturbances due to KE overrules the ergogenic potential of exogenous ketosis in endurance exercise.
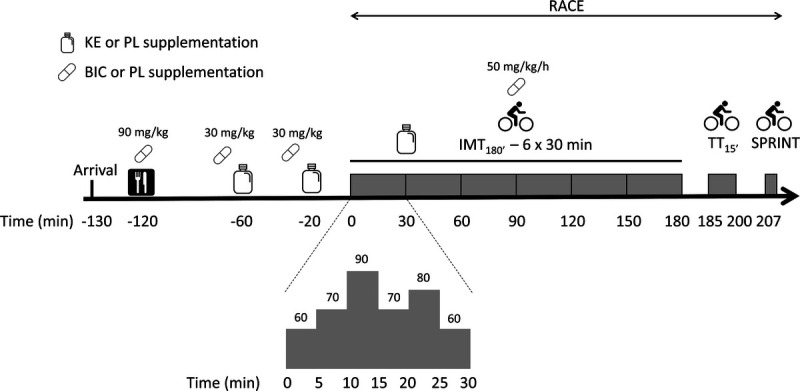
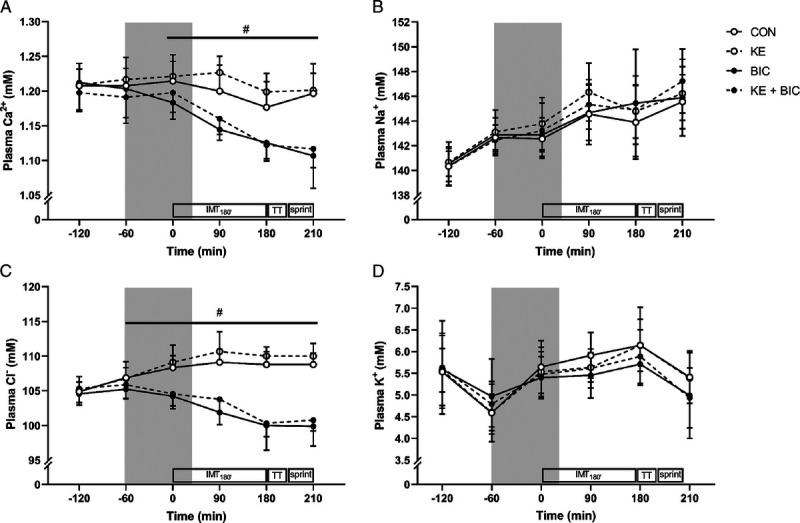
Nine well-trained male cyclists participated in a similar RACE consisting of 3 h submaximal intermittent cycling (IMT180') followed by a 15-min time trial (TT15') preceding an all-out sprint at 175% of lactate threshold (SPRINT). In a randomized crossover design, participants received (i) 65 g KE, (ii) 300 mg·kg-1 body weight NaHCO3 (BIC), (iii) KE + BIC, or (iv) a control drink (CON), together with consistent 60 g·h-1 carbohydrate intake.
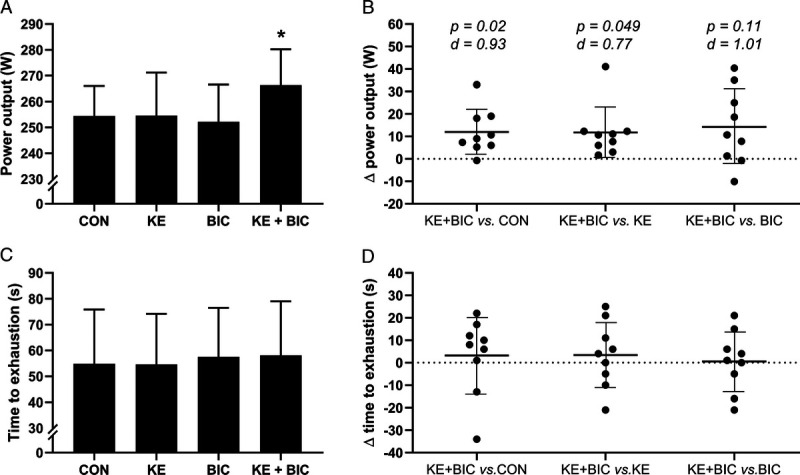
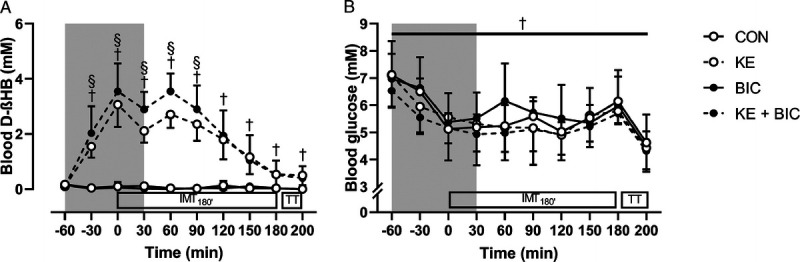
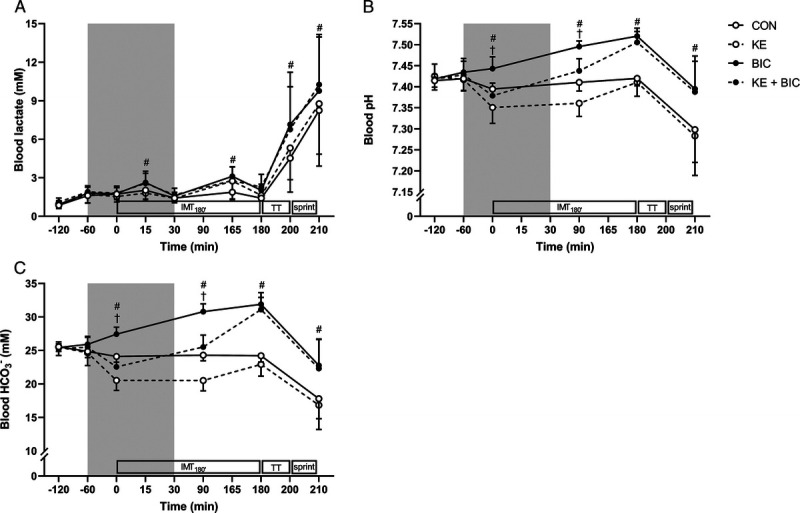
KE ingestion transiently elevated blood D-ß-hydroxybutyrate to ~2-3 mM during the initial 2 h of RACE (P < 0.001 vs CON). In KE, blood pH concomitantly dropped from 7.43 to 7.36 whereas bicarbonate decreased from 25.5 to 20.5 mM (both P < 0.001 vs CON). Additional BIC resulted in 0.5 to 0.8 mM higher blood D-ß-hydroxybutyrate during the first half of IMT180' (P < 0.05 vs KE) and increased blood bicarbonate to 31.1 ± 1.8 mM and blood pH to 7.51 ± 0.03 by the end of IMT180' (P < 0.001 vs KE). Mean power output during TT15' was similar between KE, BIC, and CON at ~255 W but was 5% higher in KE + BIC (P = 0.02 vs CON). Time to exhaustion in the sprint was similar between all conditions at ~60 s (P = 0.88). Gastrointestinal symptoms were similar between groups.
The coingestion of oral bicarbonate and KE enhances high-intensity performance at the end of an endurance exercise event without causing gastrointestinal distress.
我们最近报道,在模拟 3 小时 15 分钟的自行车比赛(RACE)的最初 30 分钟内口服酮酯(KE)摄入会暂时降低血液 pH 值和碳酸氢盐,而不会影响事件最后四分之一的最大表现。我们假设,由于 KE 导致的酸碱平衡紊乱会否定外源性酮症在耐力运动中的促能潜力。
9 名训练有素的男性自行车运动员参加了类似的 RACE,包括 3 小时的亚最大间歇骑行(IMT180'),随后进行 15 分钟的计时赛(TT15'),然后在 175%的乳酸阈值下进行全力冲刺(SPRINT)。在随机交叉设计中,参与者接受(i)65 g KE,(ii)300 mg·kg-1 体重碳酸氢钠(BIC),(iii)KE + BIC,或(iv)对照饮料(CON),同时摄入一致的 60 g·h-1 碳水化合物。
KE 摄入使血液 D-ß-羟基丁酸在 RACE 的最初 2 小时内短暂升高至~2-3 mM(与 CON 相比,P < 0.001)。在 KE 中,血液 pH 值从 7.43 降至 7.36,而碳酸氢盐从 25.5 降至 20.5 mM(均与 CON 相比,P < 0.001)。额外的 BIC 在 IMT180'的前半段导致血液 D-ß-羟基丁酸升高 0.5 至 0.8 mM(与 KE 相比,P < 0.05),并使血液碳酸氢盐升高至 31.1 ± 1.8 mM,血液 pH 值升高至 7.51 ± 0.03,在 IMT180'结束时(与 KE 相比,P < 0.001)。TT15'期间的平均功率输出在 KE、BIC 和 CON 之间相似,约为 255 W,但在 KE + BIC 中高 5%(与 CON 相比,P = 0.02)。冲刺的力竭时间在所有条件之间相似,约为 60 s(与 CON 相比,P = 0.88)。胃肠症状在各组之间相似。
口服碳酸氢盐和 KE 的共同摄入可在耐力运动结束时提高高强度运动表现,而不会引起胃肠道不适。