VA/National Clinician Scholars Program, VA Center for Clinical Management Research, VA Ann Arbor Healthcare System, Ann Arbor, Michigan.
Section of Plastic Surgery, Michigan Medicine, Ann Arbor, Michigan.
Ann Surg. 2020 Sep 1;272(3):530-536. doi: 10.1097/SLA.0000000000004201.
To examine temporal trends of OOP expenses, total payments, facility fees, and professional fees for outpatient surgery.
Approximately 48 million outpatient surgeries are performed annually with a limited financial understanding of these procedures. High OOP expenses may influence treatment decisions, delay care, and cause financial burden for patients.
We conducted a retrospective cohort study of patients with employer-sponsored insurance undergoing common outpatient surgical procedures (cholecystectomy, cataract surgery, meniscectomy, muscle/tendon procedures, and joint procedures) from 2011 to 2017. Total payments for surgical encounters paid by the insurer/employer and patient OOP expenses were calculated. We used multivariable linear regression to predict total payments and OOP expenses, with costs adjusted to the 2017 US dollar.
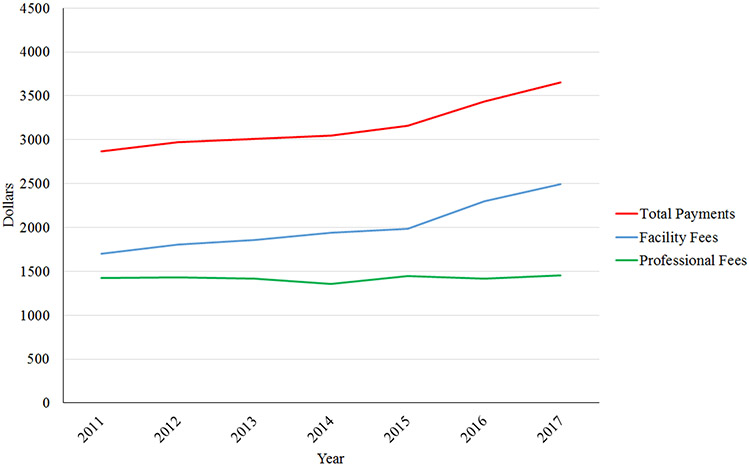
We evaluated 5,261,295 outpatient surgeries (2011-2017). Total payments increased by 29%, with a 53% increase in facility fees and no change in professional fees. OOP expenses grew by 50%. After controlling for procedure type, procedures performed in ambulatory surgery centers conferred an additional $2019 in predicted total payments (95%CI:$2002-$2036) and $324 in OOP expenses (95%CI:$319-$328) compared to predicted cost for office-based procedures. Hospital-based procedures cost an additional $2649 in predicted total payments (95%CI:$2632-$2667) and $302 in predicted OOP expenses (95%CI:$297-$306) compared to office procedures.
Increases in outpatient surgery total payments were driven primarily by facility fees and OOP expenses. OOP expenses are rising faster than total payments, highlighting the transition of costs to patients. Healthcare cost reduction policies should consider the largest areas of spending growth such as facility fees and OOP expenses to minimize the financial burden placed on patients.
考察门诊手术的自付费用、总支付额、设施费和专业费的时间趋势。
每年约有 4800 万次门诊手术,但对这些手术的财务了解有限。高额自付费用可能会影响治疗决策、延迟治疗并给患者带来经济负担。
我们对 2011 年至 2017 年期间接受常见门诊手术(胆囊切除术、白内障手术、半月板切除术、肌肉/肌腱手术和关节手术)的有雇主保险的患者进行了回顾性队列研究。计算了保险公司/雇主和患者自付费用支付的手术费用总额。我们使用多变量线性回归预测总支付额和自付费用,费用根据 2017 年的美元进行调整。
我们评估了 526.1295 万次门诊手术(2011-2017 年)。总支付额增长了 29%,其中设施费增长了 53%,专业费没有变化。自付费用增长了 50%。在控制手术类型后,与基于办公室的手术相比,在门诊手术中心进行的手术额外增加了 2019 美元的预测总支付额(95%CI:2002-2036)和 324 美元的自付费用(95%CI:319-328)。与基于办公室的手术相比,基于医院的手术在预测总支付额上额外增加了 2649 美元(95%CI:2632-2667)和 302 美元的预测自付费用(95%CI:297-306)。
门诊手术总支付额的增加主要是由设施费和自付费用推动的。自付费用的增长速度快于总支付额,突出了成本向患者转移的情况。医疗保健成本降低政策应考虑设施费和自付费用等支出增长最大的领域,以最大程度地降低患者的经济负担。