Melbourne School of Population and Global Health, The University of Melbourne, Level 5, Building 379, 207 Bouverie Street, Carlton, Victoria, 3010, Australia.
BMC Med. 2020 Aug 4;18(1):199. doi: 10.1186/s12916-020-01666-y.
In recent years, there have been adverse trends in premature cardiovascular disease (CVD) mortality rates (35-74 years) in the USA and Australia. Following long-term declines, rates in the USA are now increasing while falls in Australia have slowed rapidly. These two countries also have the highest adult obesity prevalence of high-income countries. This study investigates the role of overweight and obesity in their recent CVD mortality trends by using multiple cause of death (MCOD) data-direct individual-level evidence from death certificates-and linking the findings to cohort lifetime obesity prevalence.
We identified overweight- and obesity-related mortality as any CVD reported on the death certificate (CVD MCOD) with one or more of diabetes, chronic kidney disease, obesity, lipidemias or hypertensive heart disease (DKOLH-CVD), causes strongly associated with overweight and obesity. DKOLH-CVD comprises 50% of US and 40% of Australian CVD MCOD mortality. Trends in premature age-standardized death rates were compared between DKOLH-CVD and other CVD MCOD deaths (non-DKOLH-CVD). Deaths from 2000 to 2017 in the USA and 2006-2016 in Australia were analyzed. Trends in in age-specific DKOLH-CVD death rates were related to cohort relative lifetime obesity prevalence.
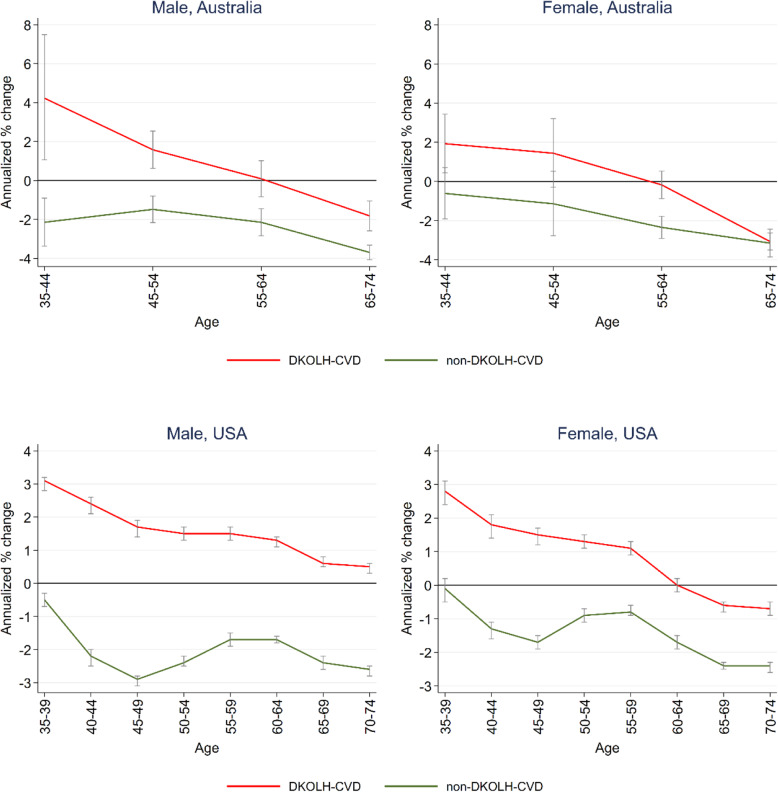
Each country's DKOLH-CVD mortality rate rose by 3% per annum in the most recent year, but previous declines had reversed more rapidly in Australia. Non-DKOLH-CVD mortality in the USA increased in 2017 after declining strongly in the early 2000s, but in Australia it has continued declining in stark contrast to DKOLH-CVD. There were larger increases in DKOLH-CVD mortality rates at successively younger ages, strongly related with higher relative lifetime obesity prevalence in younger cohorts.
The increase in DKOLH-CVD mortality in each country suggests that overweight and obesity has likely been a key driver of the recent slowdown or reversal of CVD mortality decline in both countries. The larger recent increases in DKOLH-CVD mortality and higher lifetime obesity prevalence in younger age groups are very concerning and are likely to adversely impact CVD mortality trends and hence life expectancy in future. MCOD data is a valuable but underutilized source of data to track important mortality trends.
近年来,美国和澳大利亚的 35-74 岁人群中,心血管疾病(CVD)过早死亡率呈不利趋势。美国的这一比率在经历了长期下降后,如今开始上升,而澳大利亚的下降速度则迅速放缓。这两个国家也是高收入国家中成年人肥胖症患病率最高的国家。本研究使用多种死因(MCOD)数据——直接来自死亡证明的个人层面的证据,并将研究结果与队列终身肥胖患病率相关联,以此探究超重和肥胖在两国最近 CVD 死亡率趋势中的作用。
我们将与超重和肥胖相关的死亡率定义为死亡证明中报告的任何心血管疾病(CVD MCOD),其中包括一种或多种糖尿病、慢性肾病、肥胖、血脂异常或高血压性心脏病(DKOLH-CVD),这些疾病与超重和肥胖密切相关。DKOLH-CVD 占美国 CVD MCOD 死亡率的 50%,占澳大利亚 CVD MCOD 死亡率的 40%。比较了 DKOLH-CVD 与其他 CVD MCOD 死亡(非-DKOLH-CVD)之间的早龄标准化死亡率趋势。对美国 2000 年至 2017 年和澳大利亚 2006 年至 2016 年的死亡情况进行了分析。与队列终身肥胖患病率相关联,研究了特定年龄组的 DKOLH-CVD 死亡率趋势。
在最近一年,每个国家的 DKOLH-CVD 死亡率每年上升 3%,但澳大利亚此前的下降速度更快。美国的非-DKOLH-CVD 死亡率在 21 世纪初大幅下降后,于 2017 年再次上升,但在澳大利亚,这一趋势与 DKOLH-CVD 形成鲜明对比,继续下降。DKOLH-CVD 死亡率在越来越年轻的年龄组中上升幅度更大,这与年轻队列中相对终身肥胖患病率较高密切相关。
两国的 DKOLH-CVD 死亡率上升表明,超重和肥胖很可能是两国 CVD 死亡率下降最近放缓或逆转的关键驱动因素。在最近,DKOLH-CVD 死亡率的上升幅度更大,且年轻年龄组的终身肥胖患病率更高,这令人非常担忧,可能会对未来的 CVD 死亡率趋势和预期寿命产生不利影响。MCOD 数据是一种有价值但未充分利用的数据源,可以跟踪重要的死亡率趋势。