Norwegian National Unit for Newborn Screening, Division of Paediatric and Adolescent Medicine, Oslo University Hospital, Oslo, Norway.
Paediatric Research Institute, Division of Paediatric and Adolescent Medicine, Oslo University Hospital, Oslo, Norway.
Front Immunol. 2020 Jul 9;11:1417. doi: 10.3389/fimmu.2020.01417. eCollection 2020.
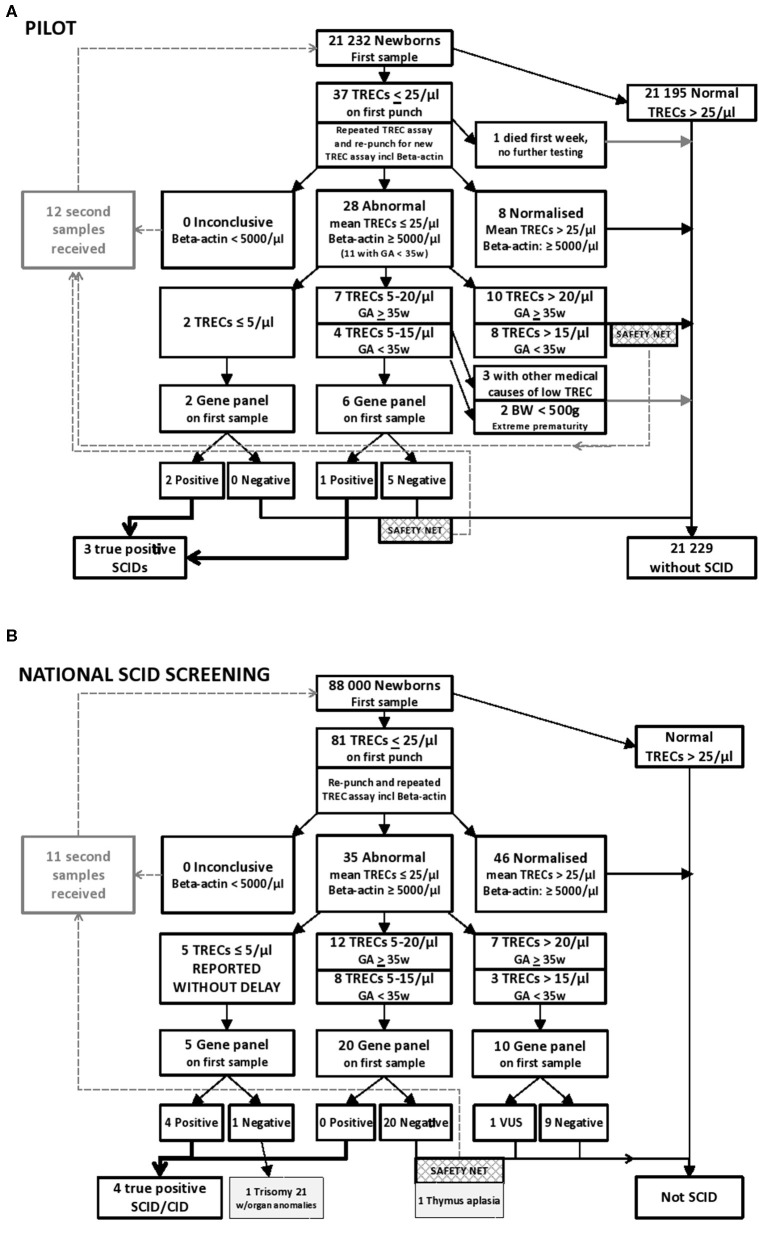
Severe combined immunodeficiency (SCID) and other T cell lymphopenias can be detected during newborn screening (NBS) by measuring T cell receptor excision circles (TRECs) in dried blood spot (DBS) DNA. Second tier next generation sequencing (NGS) with an amplicon based targeted gene panel using the same DBS DNA was introduced as part of our prospective pilot research project in 2015. With parental consent, 21 000 newborns were TREC-tested in the pilot. Three newborns were identified with SCID, and disease-causing variants in , and were confirmed by NGS on the initial DBS DNA. The molecular findings directed follow-up and therapy: the -SCID underwent early hematopoietic stem cell transplantation (HSCT) without any complications; the leaky SCID received prophylactic antibiotics, antifungals, and immunoglobulin infusions, and underwent HSCT at 1 year of age. The child with -SCID had complete Hirschsprung disease and died at 1 month of age. Since January 2018, all newborns in Norway have been offered NBS for SCID using 1st tier TRECs and 2nd tier gene panel NGS on DBS DNA. During the first 20 months of nationwide SCID screening an additional 88 000 newborns were TREC tested, and four new SCID cases were identified. Disease-causing variants in , and were molecularly confirmed on day 8, 15, 8 and 6, respectively after birth, using the initial NBS blood spot. Targeted gene panel NGS integrated into the NBS algorithm rapidly delineated the specific molecular diagnoses and provided information useful for management, targeted therapy and follow-up i.e., X rays and CT scans were avoided in the radiosensitive SCID. Second tier targeted NGS on the same DBS DNA as the TREC test provided instant confirmation or exclusion of SCID, and made it possible to use a less stringent TREC cut-off value. This allowed for the detection of leaky SCIDs, and simultaneously reduced the number of control samples, recalls and false positives. Mothers were instructed to stop breastfeeding until maternal (CMV) status was determined. Our limited data suggest that shorter time-interval from birth to intervention, may prevent breast milk transmitted CMV infection in classical SCID.
严重联合免疫缺陷(SCID)和其他 T 细胞淋巴细胞减少症可通过测量干血斑(DBS)DNA 中的 T 细胞受体切除环(TRECs)在新生儿筛查(NBS)中检测到。2015 年,作为我们前瞻性试点研究项目的一部分,引入了基于第二代测序(NGS)的二级扩增靶向基因面板,使用相同的 DBS DNA。在获得父母同意的情况下,21000 名新生儿在试点中接受了 TREC 检测。有 3 名新生儿被确定患有 SCID,通过对初始 DBS DNA 进行 NGS,发现 、 和 中的致病变异。分子发现指导了后续治疗:-SCID 患儿早期接受了造血干细胞移植(HSCT),没有任何并发症;渗漏性 SCID 患儿接受了预防性抗生素、抗真菌药和免疫球蛋白输注,并在 1 岁时接受了 HSCT。患有 -SCID 的患儿患有完全性先天性巨结肠,1 个月时死亡。自 2018 年 1 月以来,挪威所有新生儿都通过 DBS DNA 上的 1 级 TRECs 和 2 级基因面板 NGS 接受了 SCID 的 NBS。在全国性 SCID 筛查的头 20 个月中,又对 88000 名新生儿进行了 TREC 检测,发现了 4 例新的 SCID 病例。在出生后第 8、15、8 和 6 天,使用初始 NBS 血斑,在 、 和 中分别证实了致病变异,通过 NGS 进行靶向基因面板。快速描绘出特定的分子诊断,并提供了有用的管理、靶向治疗和随访信息,例如,避免了对辐射敏感的 SCID 进行 X 光和 CT 扫描。在与 TREC 检测相同的 DBS DNA 上进行二级靶向 NGS,立即确认或排除了 SCID,并可以使用较不严格的 TREC 截止值。这使得能够检测到渗漏性 SCID,同时减少了对照样本、召回和假阳性的数量。指示母亲停止母乳喂养,直到确定母亲 (CMV) 状态。我们的有限数据表明,从出生到干预的时间间隔越短,可能会防止经典 SCID 中由母乳传播的 CMV 感染。