Department of Psychiatry and Neuropsychology, Maastricht University Medical Center (MUMC+), Maastricht, the Netherlands.
Department of Internal Medicine, Maastricht University Medical Center (MUMC+), Maastricht, the Netherlands.
Diabetologia. 2020 Nov;63(11):2315-2328. doi: 10.1007/s00125-020-05247-9. Epub 2020 Aug 5.
AIMS/HYPOTHESIS: Depression is twice as common in individuals with type 2 diabetes as in the general population. However, it remains unclear whether hyperglycaemia and insulin resistance are directly involved in the aetiology of depression. Therefore, we investigated the association of markers of hyperglycaemia and insulin resistance, measured as continuous variables, with incident depressive symptoms over 4 years of follow-up.
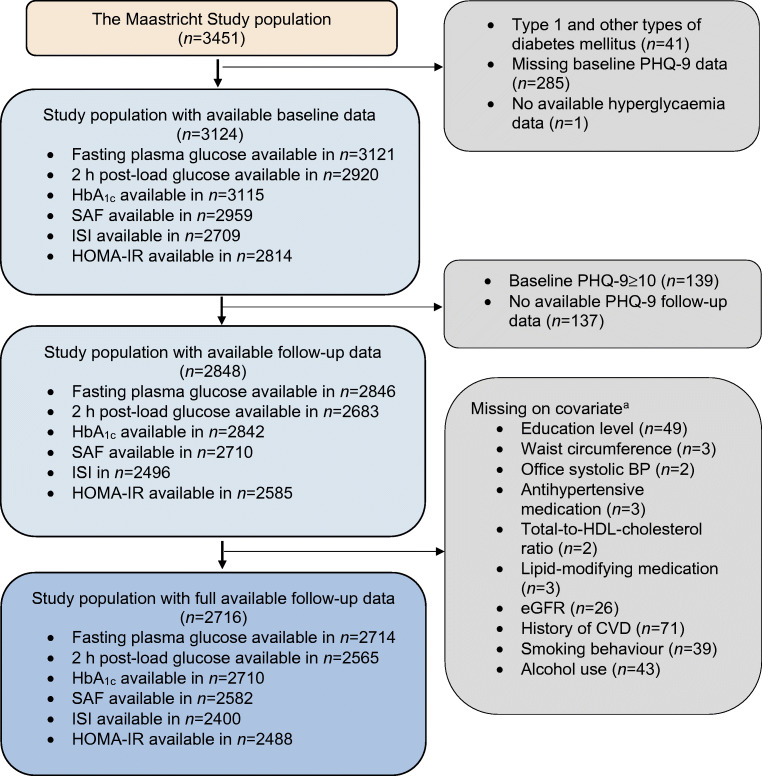
We used data from the longitudinal population-based Maastricht Study (n = 2848; mean age 59.9 ± 8.1 years, 48.8% women, 265 incident depression cases, 10,932 person-years of follow-up). We assessed hyperglycaemia by fasting and 2 h post-load OGTT glucose levels, HbA and skin autofluorescence (reflecting AGEs) at baseline. We used the Matsuda insulin sensitivity index and HOMA-IR to calculate insulin resistance at baseline. Depressive symptoms (nine-item Patient Health Questionnaire score ≥10) were assessed at baseline and annually over 4 years. We used Cox regression analyses, and adjusted for demographic, cardiovascular and lifestyle risk factors.
Fasting plasma glucose, 2 h post-load glucose and HbA levels were associated with an increased risk for incident depressive symptoms after full adjustment (HR 1.20 [95% CI 1.08, 1.33]; HR 1.25 [1.08, 1.44]; and HR 1.22 [1.09, 1.37] per SD, respectively), while skin autofluorescence, insulin sensitivity index and HOMA-IR were not (HR 0.99 [0.86, 1.13]; HR 1.02 [0.85, 1.25]; and HR 0.93 [0.81, 1.08], per SD, respectively).
CONCLUSIONS/INTERPRETATION: The observed temporal association between hyperglycaemia and incident depressive symptoms in this study supports the presence of a mechanistic link between hyperglycaemia and the development of depressive symptoms. Graphical abstract.
目的/假设:2 型糖尿病患者的抑郁发生率是普通人群的两倍。然而,高血糖和胰岛素抵抗是否直接参与抑郁的发病机制仍不清楚。因此,我们研究了连续变量测量的高血糖和胰岛素抵抗标志物与 4 年随访期间新发抑郁症状的相关性。
我们使用来自纵向人群为基础的马斯特里赫特研究(n=2848;平均年龄 59.9±8.1 岁,48.8%为女性,265 例新发抑郁症病例,10932 人年随访)的数据。我们在基线时通过空腹和 2 小时口服葡萄糖耐量试验(OGTT)血糖、HbA 和皮肤自发荧光(反映 AGEs)评估高血糖。我们使用 Matsuda 胰岛素敏感性指数和 HOMA-IR 在基线时计算胰岛素抵抗。在 4 年内,每年使用九项患者健康问卷评分(PHQ-9)≥10 评估抑郁症状。我们使用 Cox 回归分析,并调整了人口统计学、心血管和生活方式危险因素。
空腹血浆葡萄糖、2 小时 OGTT 后血糖和 HbA 水平在完全调整后与新发抑郁症状的风险增加相关(HR 1.20[95%CI 1.08,1.33];HR 1.25[1.08,1.44];和 HR 1.22[1.09,1.37]每标准差),而皮肤自发荧光、胰岛素敏感性指数和 HOMA-IR 则没有(HR 0.99[0.86,1.13];HR 1.02[0.85,1.25];和 HR 0.93[0.81,1.08],每标准差)。
结论/解释:本研究中观察到的高血糖与新发抑郁症状之间的时间相关性支持高血糖与抑郁症状发展之间存在机制联系。