Neuroscience, Brain and Mind Institute, University of Western Ontario, London, Ontario, Canada.
Psychiatry, Anatomy & Cell Biology, Brain and Mind Institute, University of Western Ontario, London, Ontario, Canada.
J Neurol Neurosurg Psychiatry. 2020 Sep;91(9):975-984. doi: 10.1136/jnnp-2020-322987. Epub 2020 Aug 7.
The clinical heterogeneity of frontotemporal dementia (FTD) complicates identification of biomarkers for clinical trials that may be sensitive during the prediagnostic stage. It is not known whether cognitive or behavioural changes during the preclinical period are predictive of genetic status or conversion to clinical FTD. The first objective was to evaluate the most frequent initial symptoms in patients with genetic FTD. The second objective was to evaluate whether preclinical mutation carriers demonstrate unique FTD-related symptoms relative to familial mutation non-carriers.
The current study used data from the Genetic Frontotemporal Dementia Initiative multicentre cohort study collected between 2012 and 2018. Participants included symptomatic carriers (n=185) of a pathogenic mutation in chromosome 9 open reading frame 72 (), progranulin () or microtubule-associated protein tau () and their first-degree biological family members (n=588). Symptom endorsement was documented using informant and clinician-rated scales.
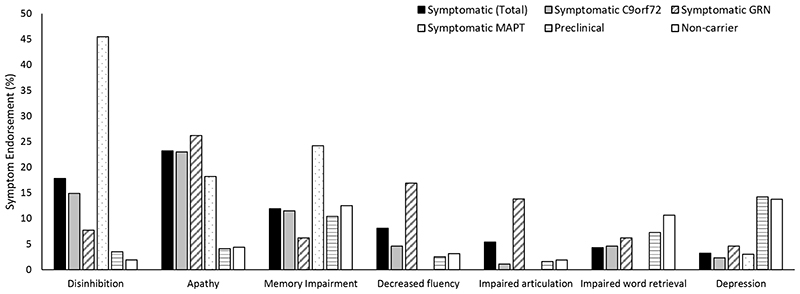
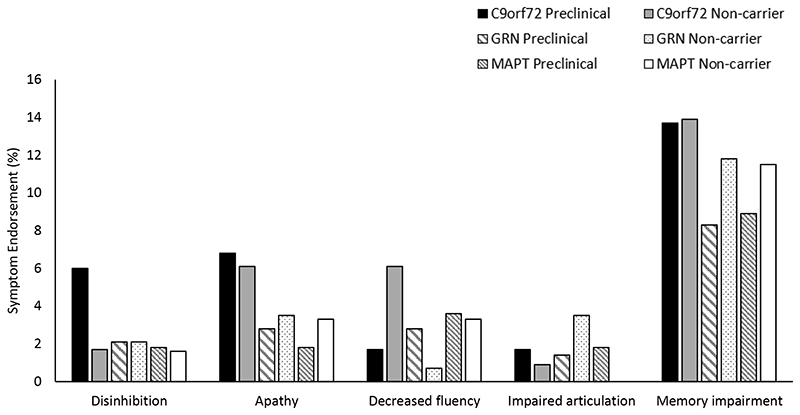
The most frequently endorsed initial symptoms among symptomatic patients were apathy (23%), disinhibition (18%), memory impairments (12%), decreased fluency (8%) and impaired articulation (5%). Predominant first symptoms were usually discordant between family members. Relative to biologically related non-carriers, preclinical carriers endorsed worse mood and sleep symptoms, and carriers endorsed marginally greater abnormal behaviours. Preclinical carriers endorsed less mood symptoms compared with non-carriers, and worse everyday skills.
Preclinical mutation carriers exhibited neuropsychiatric symptoms compared with non-carriers that may be considered as future clinical trial outcomes. Given the heterogeneity in symptoms, the detection of clinical transition to symptomatic FTD may be best captured by composite indices integrating the most common initial symptoms for each genetic group.
额颞叶痴呆(FTD)的临床异质性使得鉴定出在临床前阶段可能敏感的临床试验生物标志物变得复杂。尚不清楚临床前阶段的认知或行为变化是否可以预测遗传状态或转化为临床 FTD。第一个目标是评估遗传 FTD 患者最常见的首发症状。第二个目标是评估临床前突变携带者是否表现出与家族性突变非携带者相比独特的 FTD 相关症状。
本研究使用了 2012 年至 2018 年期间收集的遗传额颞叶痴呆倡议多中心队列研究的数据。参与者包括载有染色体 9 开放阅读框 72()、颗粒蛋白()或微管相关蛋白 tau()致病性突变的有症状携带者(n=185)及其一级生物学家庭成员(n=588)。症状的认可通过知情者和临床医生评定量表进行记录。
在有症状的患者中,最常被认可的首发症状是冷漠(23%)、抑制障碍(18%)、记忆障碍(12%)、流畅性降低(8%)和发音障碍(5%)。主要首发症状通常在家庭成员之间不一致。与生物学相关的非携带者相比,临床前 携带者表现出更严重的情绪和睡眠症状,而 携带者表现出边缘性更大的异常行为。临床前 携带者的情绪症状比非携带者轻,而日常技能更差。
与非携带者相比,临床前突变携带者表现出神经精神症状,这些症状可能被视为未来临床试验的结果。鉴于症状的异质性,对有症状 FTD 临床转变的检测可能最好通过整合每个遗传组最常见的首发症状的综合指数来捕捉。