Aslanger Emre K, Yıldırımtürk Özlem, Şimşek Barış, Bozbeyoğlu Emrah, Şimşek Mustafa Aytek, Yücel Karabay Can, Smith Stephen W, Değertekin Muzaffer
Yeditepe University Hospital, Department of Cardiology, Istanbul, Turkey.
University of Health Sciences, Dr. Siyami Ersek Thoracic and Cardiovascular Surgery Training and Research Hospital, Department of Cardiology, Istanbul, Turkey.
Int J Cardiol Heart Vasc. 2020 Jul 30;30:100603. doi: 10.1016/j.ijcha.2020.100603. eCollection 2020 Oct.
Although ST-segment elevation (STE) has been used synonymously with acute coronary occlusion (ACO), current STE criteria miss nearly one-third of ACO and result in a substantial amount of false catheterization laboratory activations. As many other electrocardiographic (ECG) findings can reliably indicate ACO, we sought whether a new ACO/non-ACO myocardial infarction (MI) paradigm would result in better identification of the patients who need acute reperfusion therapy.
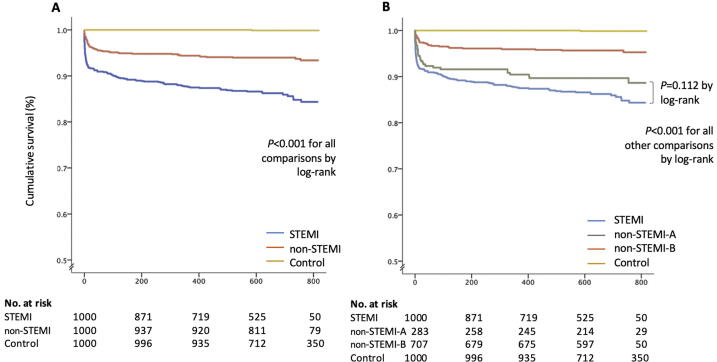
A total of 3000 patients were enrolled in STEMI, non-STEMI and control groups. All ECGs were reviewed by two cardiologists, blinded to any outcomes, for the current STEMI criteria and other subtle signs. A combined ACO endpoint was composed of peak troponin level, troponin rise within the first 24 h and angiographic appearance. The dead or alive status was checked from hospital records and from the electronic national database.
In non-STEMI group, 28.2% of the patients were re-classified by the ECG reviewers as having ACO. This subgroup had a higher frequency of ACO, myocardial damage, and both in-hospital and long-term mortality compared to non-STEMI group. A prospective ACOMI/non-ACOMI approach to the ECG had superior diagnostic accuracy compared to the STE/non-STEMI approach in the prediction of ACO and long-term mortality. In Cox-regression analysis early intervention in patients with non-ACO-predicting ECGs was associated with a higher long-term mortality.
We believe that it is time for a new paradigm shift from the STEMI/non-STEMI to the ACOMI/non-ACOMI in the acute management of MI. (DIFOCCULT study; ClinicalTrials.gov number, NCT04022668.).
尽管ST段抬高(STE)一直被视为与急性冠状动脉闭塞(ACO)同义,但目前的STE标准会遗漏近三分之一的ACO病例,并导致大量不必要的导管实验室激活。由于许多其他心电图(ECG)表现能够可靠地提示ACO,我们探讨了一种新的ACO/非ACO心肌梗死(MI)模式是否能更好地识别需要急性再灌注治疗的患者。
共纳入3000例患者,分为ST段抬高型心肌梗死(STEMI)组、非ST段抬高型心肌梗死(non-STEMI)组和对照组。两位心脏病专家在对任何结果不知情的情况下,根据当前的STEMI标准和其他细微表现对所有心电图进行评估。联合ACO终点由肌钙蛋白峰值水平、24小时内肌钙蛋白升高情况和血管造影表现组成。通过医院记录和国家电子数据库核查患者的生死状态。
在非STEMI组中,28.2%的患者经心电图评估人员重新分类为患有ACO。与非STEMI组相比,该亚组的ACO、心肌损伤以及院内和长期死亡率的发生率更高。在预测ACO和长期死亡率方面,采用前瞻性ACOMI/非ACOMI心电图评估方法比STE/非STEMI评估方法具有更高的诊断准确性。在Cox回归分析中,对预测为非ACO的心电图患者进行早期干预与更高的长期死亡率相关。
我们认为,在急性心肌梗死的管理中,是时候从STEMI/非STEMI模式向ACOMI/非ACOMI模式进行新的范式转变了。(DIFOCCULT研究;ClinicalTrials.gov编号,NCT04022668。)