Pendell Meyers H, Bracey Alexander, Lee Daniel, Lichtenheld Andrew, Li Wei J, Singer Daniel D, Rollins Zach, Kane Jesse A, Dodd Kenneth W, Meyers Kristen E, Shroff Gautam R, Singer Adam J, Smith Stephen W
Department of Emergency Medicine, Stony Brook University Hospital, Stony Brook, NY, USA.
Department of Emergency Medicine, Carolinas Medical Center, Charlotte, NC, USA.
Int J Cardiol Heart Vasc. 2021 Apr 12;33:100767. doi: 10.1016/j.ijcha.2021.100767. eCollection 2021 Apr.
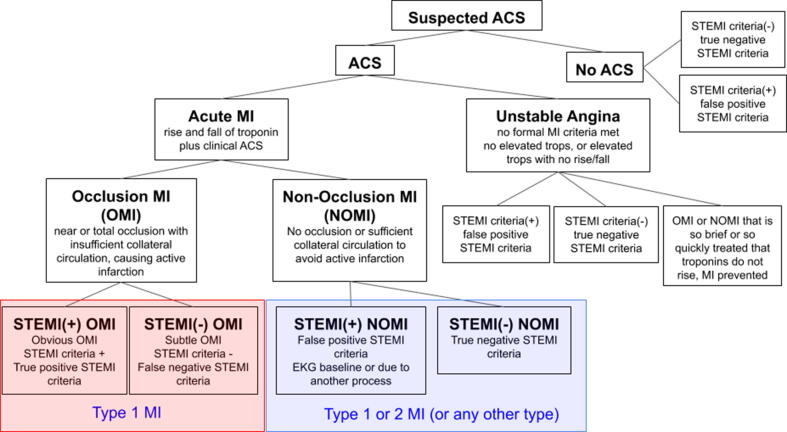
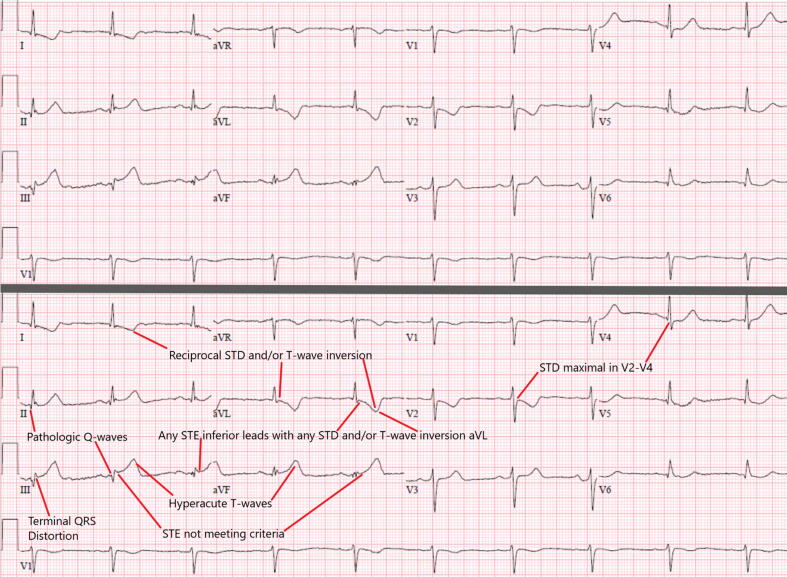
In the STEMI paradigm of Acute Myocardial Infarction (AMI), many NSTEMI patients have unrecognized acute coronary occlusion MI (OMI), may not receive emergent reperfusion, and have higher mortality than NSTEMI patients without occlusion. We have proposed a new OMI vs. Non-Occlusion MI (NOMI) paradigm shift. We sought to compare the diagnostic accuracy of OMI ECG findings vs. formal STEMI criteria for the diagnosis of OMI. We hypothesized that blinded interpretation for predefined OMI ECG findings would be more accurate than STEMI criteria for the diagnosis of OMI.
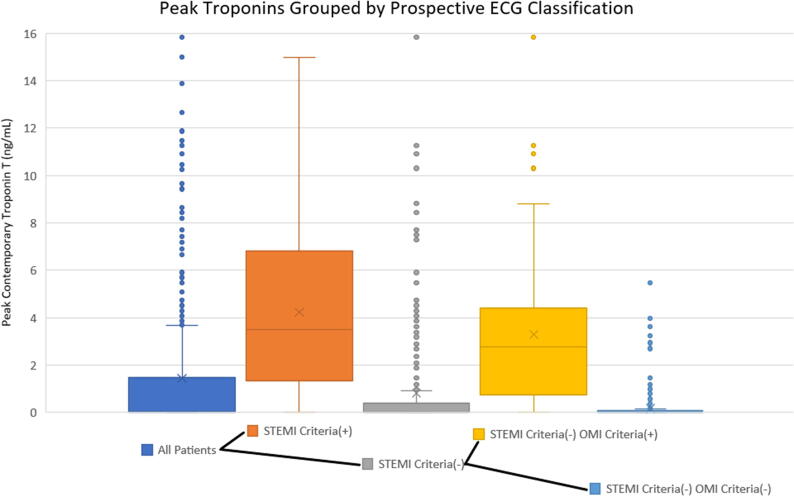
We performed a retrospective case-control study of patients with suspected acute coronary syndrome. The primary definition of OMI was either 1) acute TIMI 0-2 flow culprit or 2) TIMI 3 flow culprit with peak troponin T 1.0 ng/mL or I 10.0 ng/mL.
808 patients were included, of whom 49% had AMI (33% OMI; 16% NOMI). Sensitivity, specificity, and accuracy of STEMI criteria vs Interpreter 1 using OMI ECG findings among 808 patients were 41% vs 86%, 94% vs 91%, and 77% vs 89%, and for Interpreter 2 among 250 patients were 36% vs 80%, 91% vs 92%, and 76% vs 89%. STEMI(-) OMI patients had similar infarct size and mortality as STEMI(+) OMI patients, but greater delays to angiography.
Blinded interpretation using predefined OMI ECG findings was superior to STEMI criteria for the ECG diagnosis of Occlusion MI. These data support further investigation into the OMI vs. NOMI paradigm and suggest that STEMI(-) OMI patients could be identified rapidly and noninvasively for emergent reperfusion using more accurate ECG interpretation.
在急性心肌梗死(AMI)的ST段抬高型心肌梗死(STEMI)模式中,许多非ST段抬高型心肌梗死(NSTEMI)患者存在未被识别的急性冠状动脉闭塞性心肌梗死(OMI),可能无法接受紧急再灌注治疗,且其死亡率高于无闭塞的NSTEMI患者。我们提出了一种新的OMI与非闭塞性心肌梗死(NOMI)模式转变。我们试图比较OMI心电图表现与正式STEMI标准对OMI诊断的准确性。我们假设,对预定义的OMI心电图表现进行盲法解读在诊断OMI方面比STEMI标准更准确。
我们对疑似急性冠状动脉综合征的患者进行了一项回顾性病例对照研究。OMI的主要定义为:1)急性心肌梗死溶栓治疗(TIMI)血流0 - 2级的罪犯血管;或2)TIMI血流3级的罪犯血管且肌钙蛋白T峰值>1.0 ng/mL或肌钙蛋白I峰值>10.0 ng/mL。
纳入808例患者,其中49%患有AMI(33%为OMI;16%为NOMI)。在808例患者中,STEMI标准与使用OMI心电图表现的解读者1相比,敏感性、特异性和准确性分别为41%对86%、94%对91%、77%对89%;在250例患者中,与解读者2相比分别为36%对80%、91%对92%、76%对89%。STEMI(-)OMI患者与STEMI(+)OMI患者的梗死面积和死亡率相似,但血管造影延迟时间更长。
使用预定义的OMI心电图表现进行盲法解读在闭塞性心肌梗死的心电图诊断方面优于STEMI标准。这些数据支持对OMI与NOMI模式进行进一步研究,并表明可以通过更准确的心电图解读快速、无创地识别STEMI(-)OMI患者以进行紧急再灌注治疗。