Alencar de Pinho Natalia, Kaboré Jean, Laville Maurice, Metzger Marie, Lange Céline, Jacquelinet Christian, Combe Christian, Fouque Denis, Frimat Luc, Ayav Carol, Robinson Bruce M, Drueke Tilman, Massy Ziad A, Stengel Bénédicte
University Paris-Saclay, UVSQ, University Paris-Sud, Inserm, Clinical Epidemiology team, CESP, Villejuif, France.
Institut de Recherche en Sciences de la Santé, CNRST, Ouagadougou, Burkina Faso, Centre Muraz, Bobo-Dioulasso, Burkina Faso.
Kidney Int Rep. 2020 Jun 2;5(8):1240-1250. doi: 10.1016/j.ekir.2020.05.025. eCollection 2020 Aug.
In the general population, urinary sodium-to-potassium (uNa/K) ratio associates more strongly with high blood pressure (BP) than either urinary sodium or potassium alone. Whether this is also the case among patients with chronic kidney disease (CKD) is unknown.
We studied the associations of spot urine sodium-to-creatinine (uNa/Cr), potassium-to-creatinine (uK/Cr), and uNa/K ratios with a single office BP reading in 1660 patients with moderate to severe CKD at inclusion in the CKD-REIN cohort.
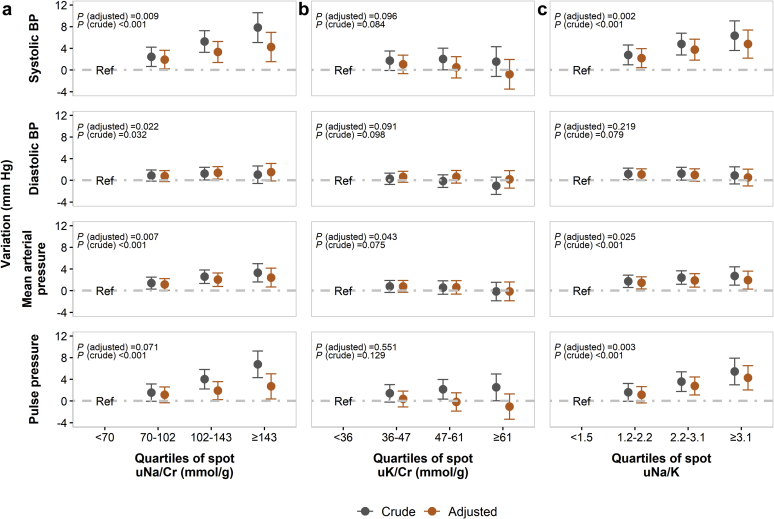
Patients' median age was 68 (interquartile range [IQR], 59-76) years; most were men (65%), had moderate CKD (57%), and albuminuria (72%). Mean systolic and diastolic BP was 142/78 mm Hg. Spot uNa/Cr and uNa/K ratios were positively associated with systolic, mean arterial, and pulse pressures. The mean adjusted difference in systolic BP between the highest and the lowest quartile (Q4 vs Q1) was 4.24 (95% confidence interval [CI], 1.53-6.96) mm Hg for uNa/Cr and 4.79 (95% CI, 2.18-7.39) mm Hg for uNa/K. Quartiles of spot uK/Cr were not associated with any BP index. The higher the quartile of uNa/K, the higher the prevalence ratio of uncontrolled (Q4 vs. Q1, 1.43; 95% CI, 1.19-1.72) or apparently treatment-resistant hypertension (Q4 vs. Q1, 1.35; 95% CI, 1.14-1.60). Findings were consistent in a subset of 803 individuals with 2 BP readings.
In patients with CKD, higher urinary sodium excretion is associated with higher BP, but unlike in general population, lower potassium excretion is not. Urinary Na/K does not add significant value in assessing high BP risk, except perhaps for hypertension control assessment.
在一般人群中,尿钠钾比(uNa/K)与高血压(BP)的关联比单独的尿钠或尿钾更强。在慢性肾脏病(CKD)患者中是否也是如此尚不清楚。
我们在CKD-REIN队列纳入的1660例中重度CKD患者中,研究了随机尿钠肌酐比(uNa/Cr)、钾肌酐比(uK/Cr)和uNa/K比与单次诊室血压读数之间的关联。
患者的年龄中位数为68岁(四分位间距[IQR],59 - 76岁);大多数为男性(65%),患有中度CKD(57%),并有蛋白尿(72%)。平均收缩压和舒张压为142/78 mmHg。随机尿uNa/Cr和uNa/K比与收缩压、平均动脉压和脉压呈正相关。uNa/Cr最高四分位数与最低四分位数(Q4与Q1)之间收缩压的平均校正差值为4.24(95%置信区间[CI],1.53 - 6.96)mmHg,uNa/K为4.79(95% CI,2.18 - 7.39)mmHg。随机尿uK/Cr的四分位数与任何血压指标均无关联。uNa/K的四分位数越高,血压控制不佳(Q4与Q1,1.43;95% CI,1.19 - 1.72)或明显难治性高血压(Q4与Q1,1.35;95% CI,1.14 - 1.60)的患病率比越高。在803例有两次血压读数的亚组中,结果一致。
在CKD患者中,较高的尿钠排泄与较高的血压相关,但与一般人群不同的是,较低的尿钾排泄并非如此。尿Na/K在评估高血压风险方面没有增加显著价值,可能除了用于高血压控制评估外。