Stengel Bénédicte, Muenz Daniel, Tu Charlotte, Speyer Elodie, Alencar de Pinho Natalia, Combe Christian, Yamagata Kunihiro, Reichel Helmut, Fliser Danilo, Massy Ziad A, Lopes Antonio A, Jadoul Michel, Winkelmayer Wolfgang C, Pisoni Ronald L, Robinson Bruce M, Pecoits-Filho Roberto
Centre for Research in Epidemiology and Population Health, Paris-Saclay University, Versailles Saint Quentin University, INSERM UMRS 1018, Villejuif, France.
Arbor Research Collaborative for Health, Ann Arbor, Michigan, USA.
Kidney Int Rep. 2020 Dec 17;6(2):437-448. doi: 10.1016/j.ekir.2020.11.039. eCollection 2021 Feb.
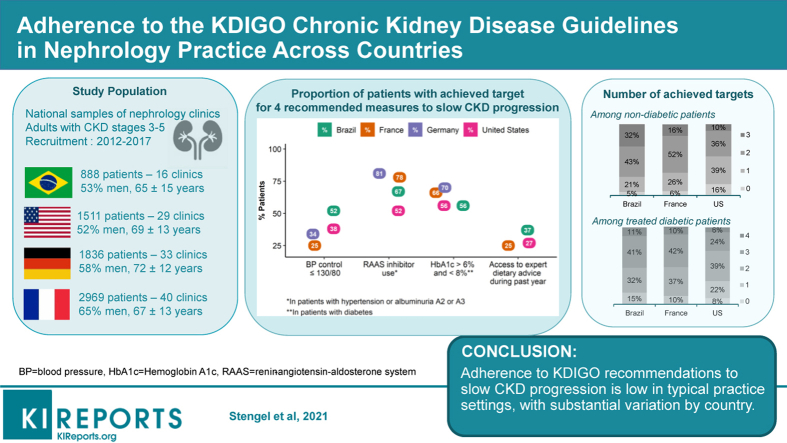
The uptake of the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 chronic kidney disease (CKD) Guideline is not fully described in real-world nephrology practice across the world.
We used baseline data from the CKD Outcomes and Practice Patterns Study (2013-2017), a 4-country cohort of patients with estimated glomerular filtration rate <60 ml/min per 1.73 m recruited from national samples of nephrology clinics, to describe adherence to measures for monitoring and delaying CKD progression. Data were collected as in clinical practice, except laboratory measures per protocol in France.
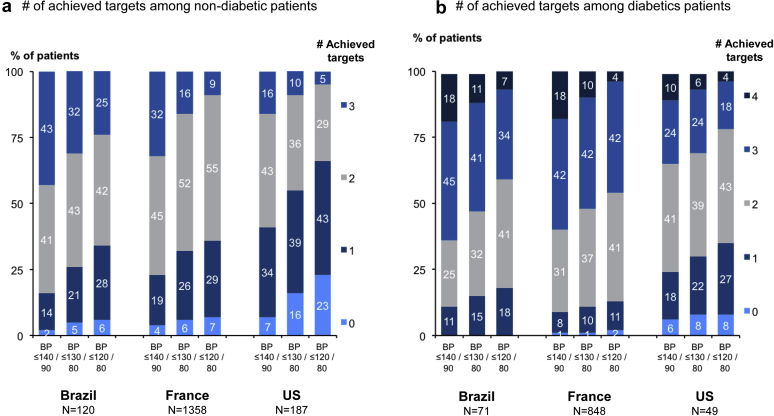
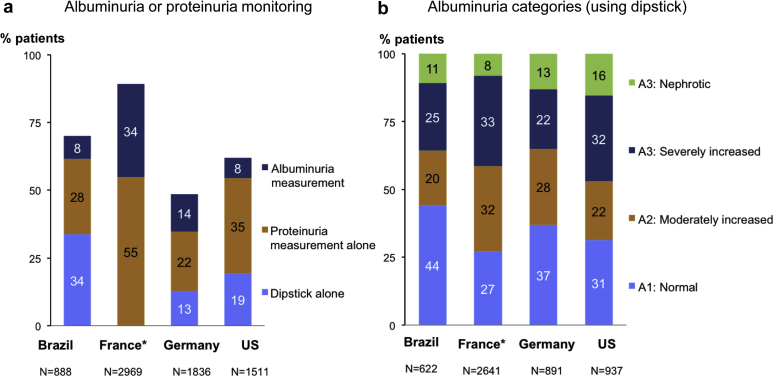
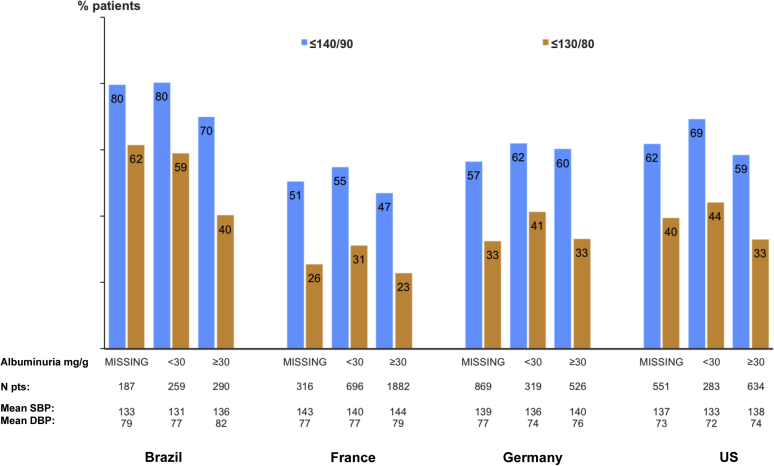
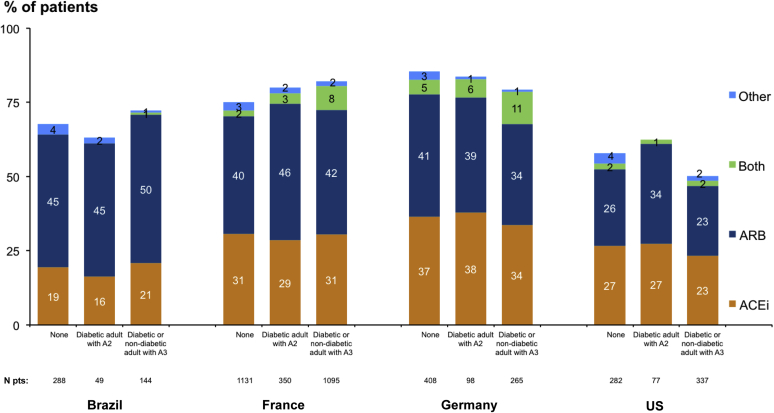
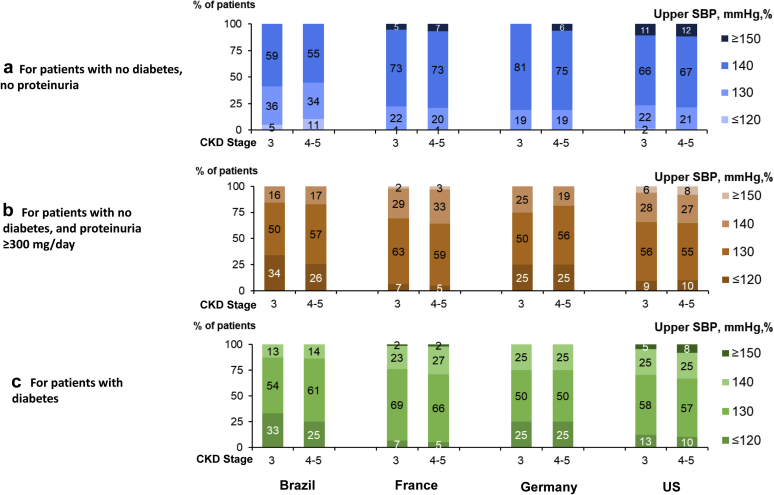
The mean age ranged from 65 years in Brazil to 72 years in Germany. Albuminuria (mostly proteinuria) was measured routinely in 36% to 43% of patients in Brazil, Germany, and the United States. Blood pressure control (≤140/90 mm Hg) ranged from 49% in France to 76% in Brazil; <40% of patients had blood pressure ≤130/80 mm Hg everywhere but Brazil (52%). More than 40% of nephrologists in Brazil reported a systolic blood pressure target ≤130 mm Hg for nondiabetic patients without proteinuria, but only 19% to 24% elsewhere. Prescription of renin-angiotensin aldosterone system inhibitors ranged from 52% in the United States to 81% in Germany. Dietary advice was more frequent for salt than protein intake; dietitian visits were uncommon. In nondiabetic patients, achievement of all 3 targets including blood pressure ≤130/80 mm Hg, renin-angiotensin aldosterone system inhibition, and dietary advice, ranged from 10% in the United States to 32% in Brazil; in treated diabetic patients, this ranged from 6% to 11% after including hemoglobin A1c target.
Adherence to recommendations to slow CKD progression is low in typical practice settings, and substantial variation among countries for some indicates opportunities for improvement.
《改善全球肾脏病预后(KDIGO)2012慢性肾脏病(CKD)指南》在全球实际肾脏病诊疗实践中的应用情况尚未得到充分描述。
我们使用了慢性肾脏病预后与实践模式研究(2013 - 2017年)的基线数据,该研究是一项涉及4个国家的队列研究,从肾脏病诊所的全国样本中招募估算肾小球滤过率低于60 ml/(min·1.73 m²)的患者,以描述对监测和延缓CKD进展措施的依从性。数据收集方式与临床实践相同,但法国按照方案进行实验室检测。
平均年龄从巴西的65岁到德国的72岁不等。在巴西、德国和美国,36%至43%的患者常规检测蛋白尿(大多为蛋白尿)。血压控制(≤140/90 mmHg)从法国的49%到巴西的76%不等;除巴西(52%)外,各地血压≤130/80 mmHg的患者均不到40%。巴西超过40%的肾脏病医生报告,无蛋白尿的非糖尿病患者收缩压目标≤130 mmHg,但其他地区仅为19%至24%。肾素 - 血管紧张素 - 醛固酮系统抑制剂的处方率从美国的52%到德国的81%不等。关于盐摄入的饮食建议比蛋白质摄入更为常见;营养师会诊并不常见。在非糖尿病患者中,实现所有3个目标(包括血压≤130/80 mmHg、肾素 - 血管紧张素 - 醛固酮系统抑制和饮食建议)的比例从美国的10%到巴西的32%不等;在接受治疗的糖尿病患者中(纳入糖化血红蛋白目标后),这一比例为6%至11%。
在典型的实践环境中,对延缓CKD进展建议的依从性较低,一些国家之间的显著差异表明存在改进空间。