International Institute for Population Sciences (IIPS), Mumbai, India.
School of Health and Environmental Studies, Hamdan Bin Mohammed Smart University, Dubai, United Arab Emirates.
BMC Public Health. 2020 Aug 10;20(1):1221. doi: 10.1186/s12889-020-09321-0.
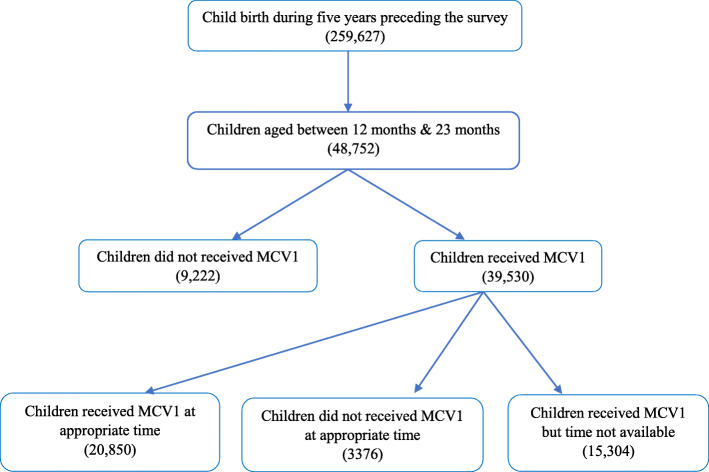
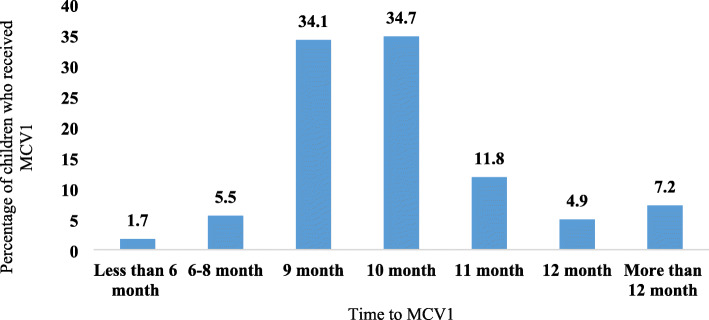
Between 2010 and 2018, measles-related mortality had halved in India mainly with effective measles vaccination campaigns and widespread coverage across the states and population subgroups. Despite the commendable vaccination coverage, 2.9 million children in India missed the first dose of measles vaccine (MCV1) in 2017, and many of those vaccinated were not vaccinated at the recommended age (i.e. between 9 and 12 months). This study analyzed pattern and correlates of MCV1 coverage and MCV1 administration at recommended age among children aged 12-23 months in India.
We used the official data from the recent round of National Family Health Survey (NFHS-4), a nationally representative cross-sectional household survey in India conducted in 2015-16. Descriptive statistics and logistic regression analysis were applied to ascertain the influence of specified socio-demographic variables affecting measles vaccination coverage in India.
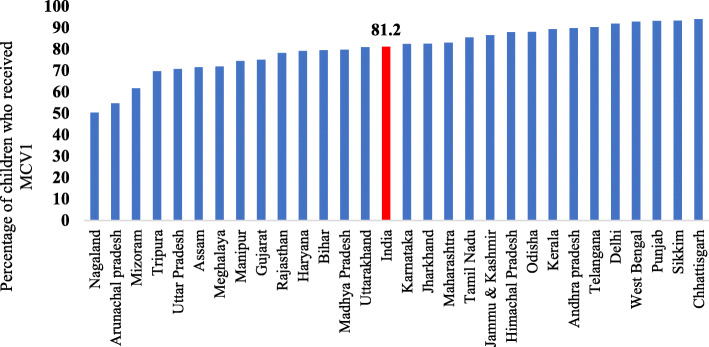
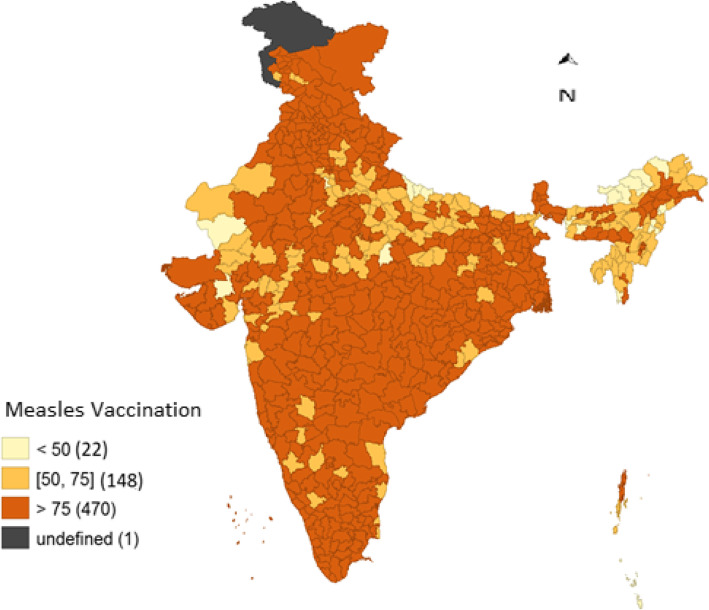
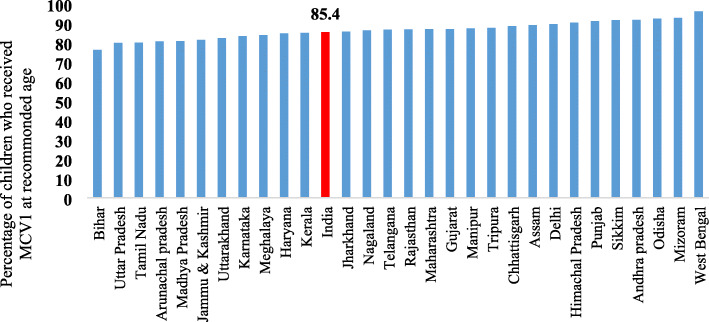
The study revealed the distinct variations in coverage of MCV1 between the districts of India. There were also major challenges with age recommended vaccination, with about 15% of eligible children not vaccinated within the recommended age range, attributable to several socio-demographic factors. Significantly, antenatal care utilization of mothers strongly influenced MCV1 coverage and age recommended MCV1 coverage in India. The study also identified that children who missed MCV1 had one or more adverse health risks such as malnutrition, anemia and diarrhea disease.
A socio-economic gradient exists in India's MCV1 coverage, mediated by antenatal visits, education of mothers, and highlighted socio-demographic factors. Infection with measles was significantly correlated with greater anthropometric deficits among the study cohort, indicating a wider range of benefits from preventing measles infection. Eliminating morbidity and mortality from measles in India is feasible, although it will require efficient expanded program on immunization management, enhanced health literacy among mothers, continuing commitment from central state and district political authorities.
2010 年至 2018 年期间,印度的麻疹相关死亡率减半,这主要得益于有效的麻疹疫苗接种运动以及在各州和人口亚群中的广泛覆盖。尽管疫苗接种覆盖率值得称赞,但 2017 年印度仍有 290 万名儿童错过第一剂麻疹疫苗(MCV1)接种,而且许多已接种疫苗的儿童并未在推荐年龄(即 9 至 12 个月)接种疫苗。本研究分析了印度 12-23 个月儿童 MCV1 覆盖率和推荐年龄 MCV1 接种的模式和相关因素。
我们使用了来自最近一轮全国家庭健康调查(NFHS-4)的官方数据,这是印度于 2015-16 年进行的一项具有全国代表性的横断面家庭调查。我们应用描述性统计和逻辑回归分析来确定影响印度麻疹疫苗接种覆盖率的特定社会人口学变量的影响。
研究表明,印度各地区 MCV1 覆盖率存在明显差异。在推荐年龄接种方面也存在重大挑战,大约 15%的符合条件的儿童未在推荐年龄范围内接种疫苗,这归因于几个社会人口学因素。重要的是,母亲的产前保健利用强烈影响印度的 MCV1 覆盖率和推荐年龄的 MCV1 覆盖率。研究还发现,错过 MCV1 接种的儿童存在一个或多个不良健康风险,如营养不良、贫血和腹泻疾病。
印度的 MCV1 覆盖率存在社会经济梯度,这是由产前检查、母亲教育以及突出的社会人口学因素介导的。在研究队列中,麻疹感染与更大的人体测量缺陷显著相关,这表明预防麻疹感染的益处更为广泛。尽管这需要有效的扩大免疫规划管理、提高母亲的健康素养、中央州和地区政治当局的持续承诺,但在印度消除麻疹的发病率和死亡率是可行的。