Lothian Birth Cohorts, School of Philosophy, Psychology & Language Sciences, 7 George Square, University of Edinburgh, Edinburgh, UK.
Edinburgh Dementia Prevention, University of Edinburgh, BioCube 1, Edinburgh, UK.
Exp Gerontol. 2020 Oct 1;139:111055. doi: 10.1016/j.exger.2020.111055. Epub 2020 Aug 11.
Research suggests that frailty is associated with higher inflammation levels. We investigated the longitudinal association between chronic inflammation and frailty progression.
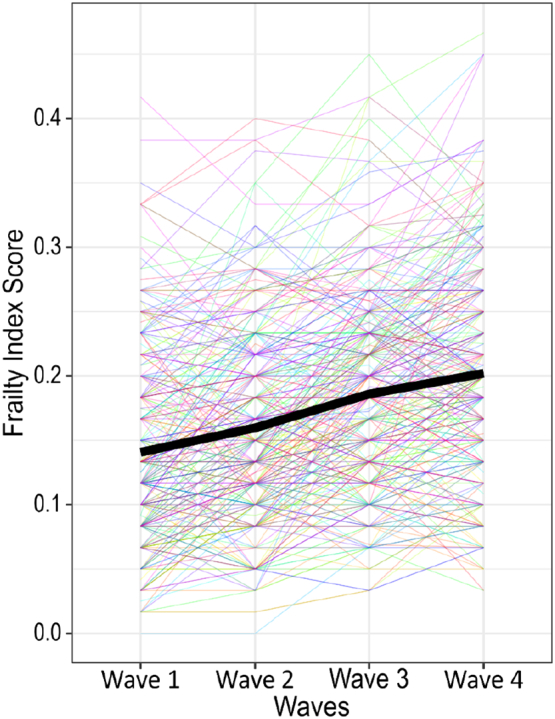
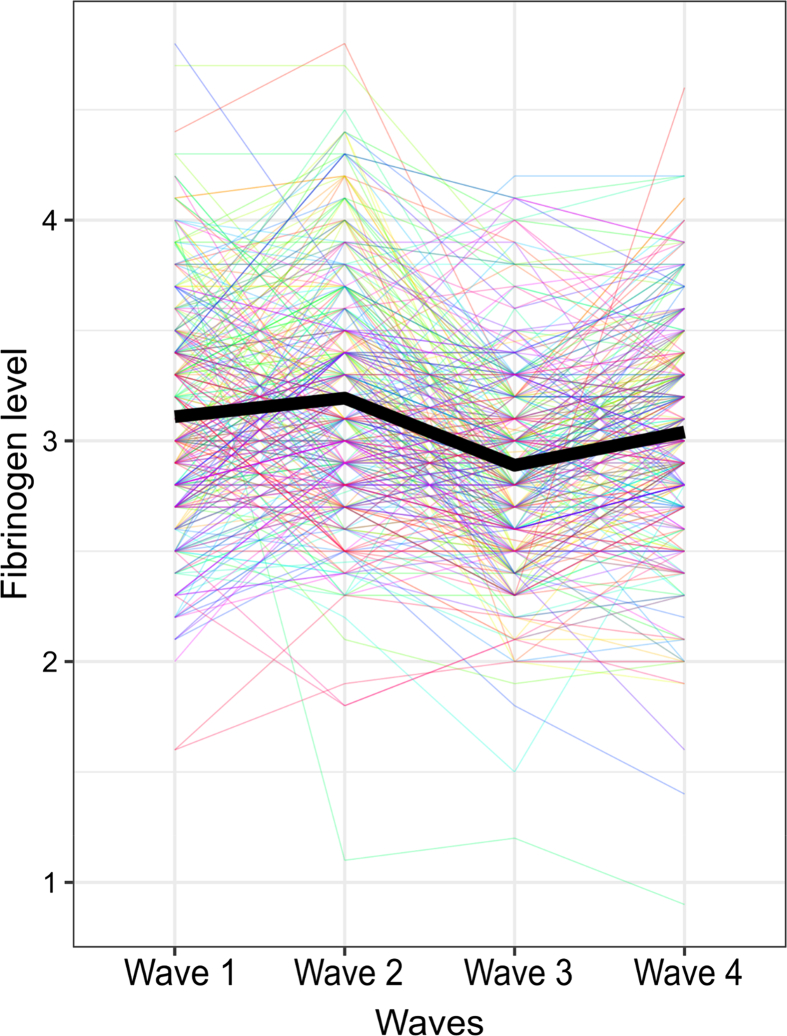
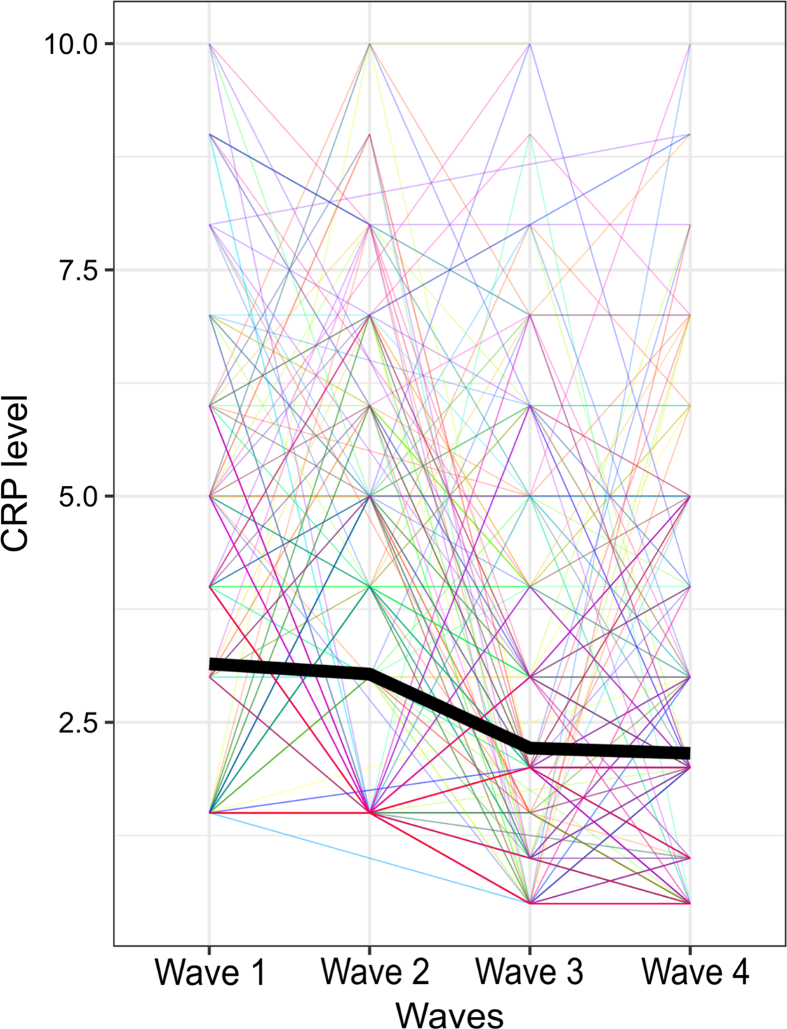
Participants of the Lothian Birth Cohort 1936, aged 70 at baseline were tested four times over 12 years (wave 1: n = 1091, wave 4: n = 550). Frailty was assessed by; the Frailty Index at waves 1-4 and Fried phenotype at waves 1, 3 and 4. Two blood-based inflammatory biomarkers were measured at wave 1: Fibrinogen and C-reactive protein (CRP).
Fully-adjusted, linear mixed effects models showed higher Fibrinogen was significantly associated with higher wave 1 Frailty Index score (β = 0.011, 95% CI[0.002,0.020], p < .05). Over 12 year follow-up, higher wave 1 CRP (β = 0.001, 95% CI[0.000,0.002], p < .05) and Fibrinogen (β = 0.004, 95% CI[0.001,0.007], p < .05) were significantly associated with increased Frailty Index change. For the Fried phenotype, wave 1 Pre-frail and Frail participants had higher CRP and Fibrinogen than Non-frail participants (p < .001). Logistic regression models calculated risk of worsening frailty over follow-up and we observed no significant association of CRP or Fibrinogen in minimally-adjusted nor fully-adjusted models.
Findings showed a longitudinal association of higher wave 1 CRP and Fibrinogen on worsening frailty in the Frailty Index, but not Fried Phenotype. A possible explanation for this disparity may lie in the conceptual differences between frailty measures (a biopsychosocial vs physical approach). Future research, which further explores different domains of frailty, as well the associations between improving frailty and inflammation levels, may elucidate the pathway through which inflammation influences frailty progression. This may improve earlier identification of those at high frailty risk.
研究表明,衰弱与更高的炎症水平有关。我们研究了慢性炎症与衰弱进展之间的纵向关联。
洛锡安出生队列 1936 年的参与者,在基线时年龄为 70 岁,在 12 年内进行了四次测试(第 1 波:n=1091,第 4 波:n=550)。在第 1-4 波通过衰弱指数评估衰弱情况,在第 1、3 和 4 波通过 Fried 表型评估衰弱情况。在第 1 波时测量了两种基于血液的炎症生物标志物:纤维蛋白原和 C 反应蛋白(CRP)。
经过充分调整的线性混合效应模型显示,较高的纤维蛋白原与较高的第 1 波衰弱指数评分显著相关(β=0.011,95%CI[0.002,0.020],p<.05)。在 12 年的随访期间,较高的第 1 波 CRP(β=0.001,95%CI[0.000,0.002],p<.05)和纤维蛋白原(β=0.004,95%CI[0.001,0.007],p<.05)与衰弱指数变化增加显著相关。对于 Fried 表型,第 1 波的前期虚弱和虚弱参与者的 CRP 和纤维蛋白原高于非虚弱参与者(p<.001)。我们观察到,在最小调整和完全调整的模型中,CRP 或纤维蛋白原与随访中衰弱恶化的风险没有显著关联。
研究结果表明,较高的第 1 波 CRP 和纤维蛋白原与衰弱指数的衰弱恶化呈纵向关联,但与 Fried 表型无关。造成这种差异的一个可能原因在于衰弱测量方法(生物心理社会与身体方法)之间的概念差异。未来的研究进一步探索不同领域的衰弱以及改善衰弱与炎症水平之间的关联,可能会阐明炎症影响衰弱进展的途径。这可能会提高对高衰弱风险人群的早期识别。