Bergman Martin J, Kivitz Alan J, Pappas Dimitrios A, Kremer Joel M, Zhang Lixia, Jeter Anna, Withers Johanna B
Drexel University College of Medicine, Philadelphia, PA, USA.
Department of Rheumatology, Altoona Center for Clinical Research, Duncansville, PA, USA.
Rheumatol Ther. 2020 Dec;7(4):775-792. doi: 10.1007/s40744-020-00226-3. Epub 2020 Aug 14.
The PrismRA test identifies rheumatoid arthritis (RA) patients who are unlikely to respond to anti-tumor necrosis factor (anti-TNF) therapies. This study evaluated the clinical and financial outcomes of incorporating PrismRA into routine clinical care of RA patients.
A decision-analytic model was created to evaluate clinical and economic outcomes in the 12-month period following first biologic treatment. Two treatment strategies were compared: (1) observed clinical decision-making based on a 175-patient cohort receiving an anti-TNF therapy as their first biologic after failure of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and (2) modeled clinical decision-making of the same population using PrismRA results to inform first-line biologic treatment choice. Modeled costs include biologic drug pharmacy, non-biologic pharmacy, and total medical costs. The odds of inadequate response to anti-TNF therapies and various components of patient care were calculated based on PrismRA results.
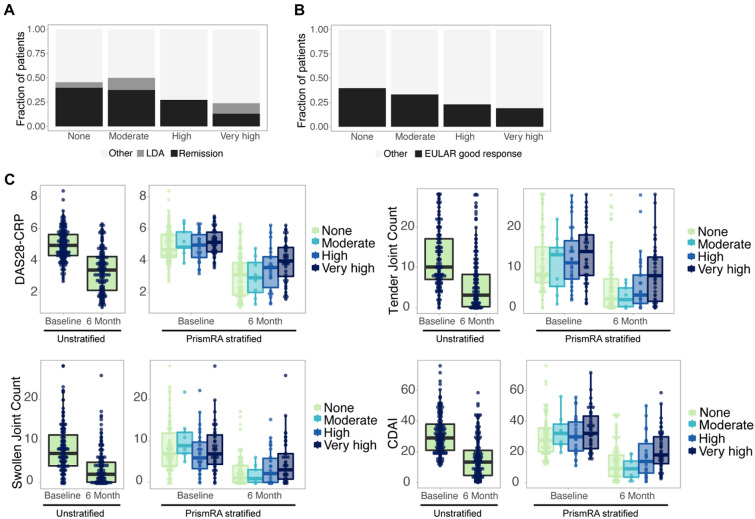
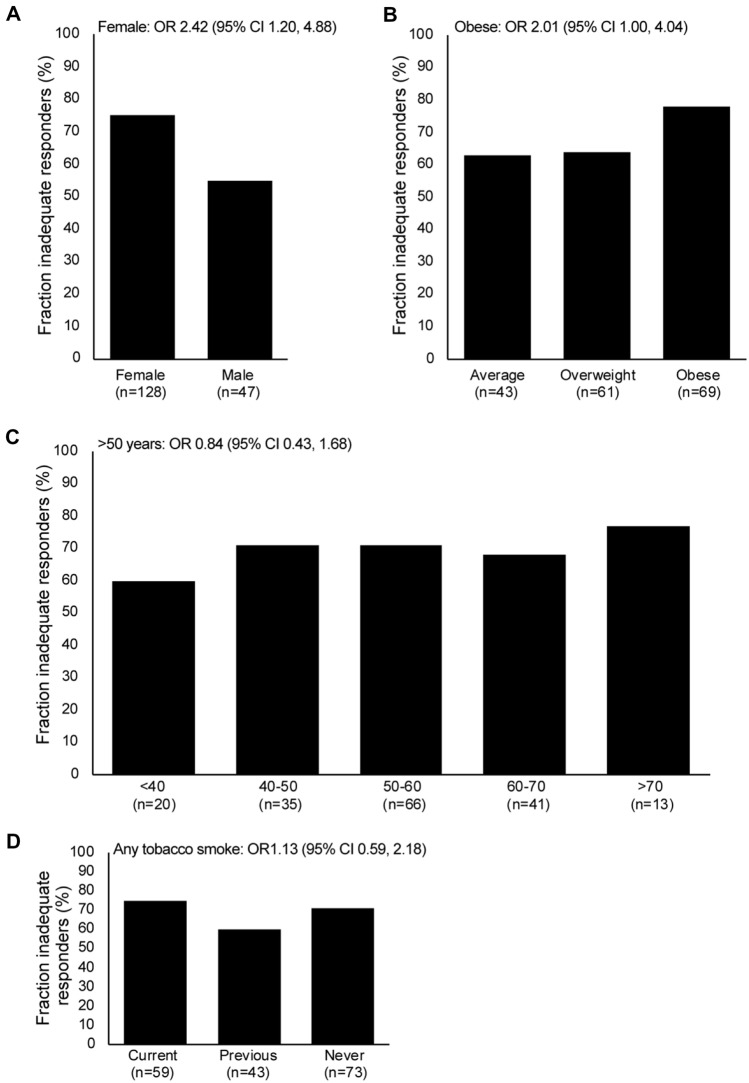
Identifying predicted inadequate responders to anti-TNF therapies resulted in a modeled 38% increase in ACR50 response to first-line biologic therapies. The fraction of patients who achieved an ACR50 response to any therapy (TNFi and others) within the 12-month period was 33% higher in the PrismRA-stratified population than in the unstratified population (59 vs. 44%, respectively). When therapy prescriptions were modeled according to PrismRA results, cost savings were modeled for all financial variables: overall costs (4% decreased total, 19% decreased on ineffective treatments), total biologic drug pharmacy (4% total, 23% ineffective), non-biologic pharmacy (2% total, 19% ineffective), and medical costs (6% total, 19% ineffective). Female sex was the clinical metric that showed the greatest association with inadequate response to anti-TNF therapies (odds ratio 2.42, 95% confidence interval 1.20, 4.88).
If PrismRA is implemented into routine clinical care as modeled, predicting which RA patients will have an inadequate response to anti-TNF therapies could save > $7 million in overall ineffective healthcare costs per 1000 patients tested and increase targeted DMARD response rates in RA.
PrismRA检测可识别出不太可能对抗肿瘤坏死因子(抗TNF)疗法产生反应的类风湿关节炎(RA)患者。本研究评估了将PrismRA纳入RA患者常规临床护理的临床和经济结果。
建立了一个决策分析模型,以评估首次生物治疗后12个月内的临床和经济结果。比较了两种治疗策略:(1)基于175名患者队列的观察性临床决策,这些患者在传统合成改善病情抗风湿药物(csDMARDs)治疗失败后,接受抗TNF疗法作为其首次生物治疗;(2)使用PrismRA结果为同一人群的一线生物治疗选择提供信息的模拟临床决策。模拟成本包括生物药物药房、非生物药物药房和总医疗成本。根据PrismRA结果计算对抗TNF疗法反应不足的几率以及患者护理的各个组成部分。
识别出对抗TNF疗法预测反应不足的患者,模拟显示一线生物治疗的ACR50反应增加了38%。在12个月内对任何疗法(TNFi和其他疗法)达到ACR50反应的患者比例,在PrismRA分层人群中比未分层人群高33%(分别为59%和44%)。当根据PrismRA结果模拟治疗处方时,所有财务变量均显示成本节约:总成本(降低4%,无效治疗降低19%)、生物药物药房总成本(降低4%,无效治疗降低23%)、非生物药物药房(降低2%,无效治疗降低19%)和医疗成本(降低6%,无效治疗降低19%)。女性是与抗TNF疗法反应不足关联最大的临床指标(优势比2.42,95%置信区间1.20,4.88)。
如果按照模拟将PrismRA应用于常规临床护理,预测哪些RA患者对抗TNF疗法反应不足,每检测1000名患者可节省超过700万美元的总体无效医疗成本,并提高RA中靶向DMARD的反应率。