Lessing Noah L, Zuckerman Scott L, Lazaro Albert, Leech Ashley A, Leidinger Andreas, Rutabasibwa Nicephorus, Shabani Hamisi K, Mangat Halinder S, Härtl Roger
University of Maryland School of Medicine, Baltimore, MD, USA.
12328Vanderbilt University Medical Center, Nashville, TN, USA.
Global Spine J. 2022 Jan;12(1):15-23. doi: 10.1177/2192568220944888. Epub 2020 Aug 17.
Retrospective cost-effectiveness analysis.
While the incidence of traumatic spine injury (TSI) is high in low-middle income countries (LMICs), surgery is rarely possible due to cost-prohibitive implants. The objective of this study was to conduct a preliminary cost-effectiveness analysis of operative treatment of TSI patients in a LMIC setting.
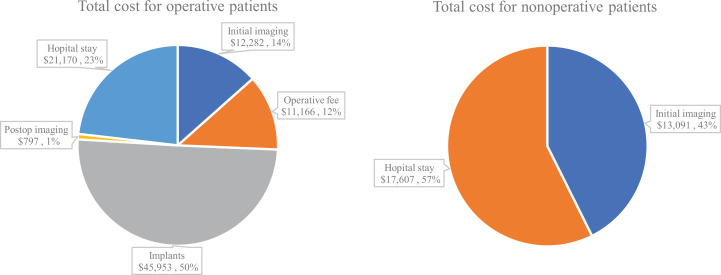
At a tertiary hospital in Tanzania from September 2016 to May 2019, a retrospective analysis was conducted to estimate the cost-effectiveness of operative versus nonoperative treatment of TSI. Operative treatment included decompression/stabilization. Nonoperative treatment meant 3 months of bed rest. Direct costs included imaging, operating fees, surgical implants, and length of stay. Four patient scenarios were chosen to represent the heterogeneity of spine trauma: Quadriplegic, paraplegic, neurologic improvement, and neurologically intact. Disability-adjusted-life-years (DALYs) and incremental-cost-effectiveness ratios were calculated to determine the cost per unit benefit of operative versus nonoperative treatment. was the primary outcome (i.e., the amount of money required to avoid losing 1 year of healthy life).
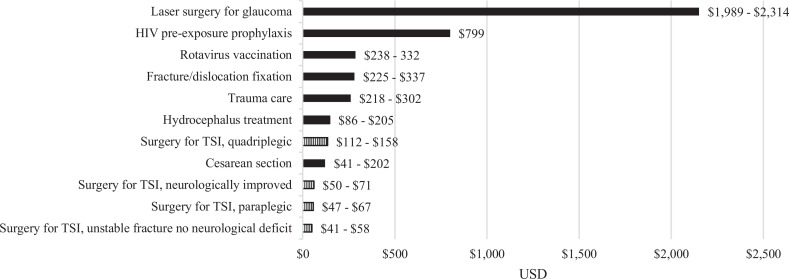
A total of 270 TSI patients were included (125 operative; 145 nonoperative). Operative treatment averaged $731/patient. Nonoperative care averaged $212/patient. Comparing operative versus nonoperative treatment, the incremental for each patient outcome was: quadriplegic ($112-$158/DALY averted), paraplegic ($47-$67/DALY averted), neurologic improvement ($50-$71/DALY averted), neurologically intact ($41-$58/DALY averted). Sensitivity analysis confirmed these findings without major differences.
This preliminary cost-effectiveness analysis suggests that the upfront costs of spine trauma surgery may be offset by a reduction in disability. LMIC governments should consider conducting more spine trauma cost-effectiveness analyses and including spine trauma surgery in universal health care.
回顾性成本效益分析。
虽然中低收入国家(LMICs)创伤性脊柱损伤(TSI)的发病率很高,但由于植入物成本过高,很少能够进行手术。本研究的目的是在中低收入国家背景下对TSI患者的手术治疗进行初步成本效益分析。
2016年9月至2019年5月在坦桑尼亚的一家三级医院进行回顾性分析,以评估TSI手术治疗与非手术治疗的成本效益。手术治疗包括减压/稳定术。非手术治疗意味着卧床休息3个月。直接成本包括影像学检查、手术费用、手术植入物和住院时间。选择四种患者情况来代表脊柱创伤的异质性:四肢瘫痪、截瘫、神经功能改善和神经功能正常。计算伤残调整生命年(DALYs)和增量成本效益比,以确定手术治疗与非手术治疗的单位效益成本。是主要结果(即避免失去1年健康生命所需的资金量)。
共纳入270例TSI患者(125例手术治疗;145例非手术治疗)。手术治疗平均每位患者731美元。非手术治疗平均每位患者212美元。比较手术治疗与非手术治疗,每种患者结果的增量为:四肢瘫痪(避免每DALY 112 - 158美元)、截瘫(避免每DALY 47 - 67美元)、神经功能改善(避免每DALY 50 - 71美元)、神经功能正常(避免每DALY 41 - 58美元)。敏感性分析证实了这些发现,且无重大差异。
这项初步成本效益分析表明,脊柱创伤手术的前期成本可能因残疾减少而得到抵消。中低收入国家政府应考虑开展更多脊柱创伤成本效益分析,并将脊柱创伤手术纳入全民医疗保健。