Marseille Elliot, Jiwani Aliya, Raut Abhishek, Verguet Stéphane, Walson Judd, Kahn James G
Health Strategies International, Oakland, California, USA.
Health Strategies International, Arlington, Virginia, USA.
BMJ Open. 2014 Jun 26;4(6):e003987. doi: 10.1136/bmjopen-2013-003987.
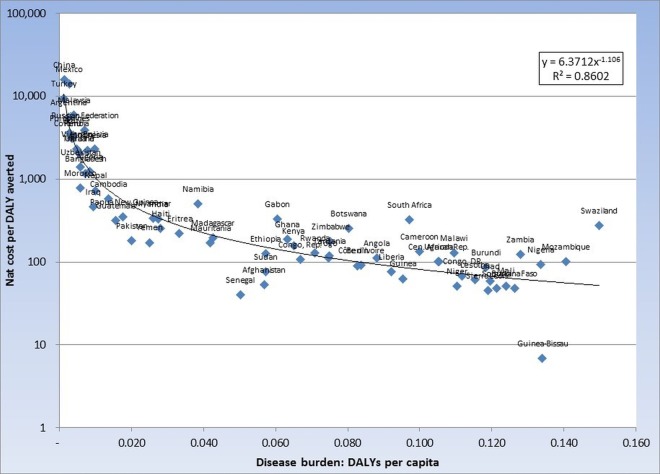
This study estimated the health impact, cost and cost-effectiveness of an integrated prevention campaign (IPC) focused on diarrhoea, malaria and HIV in 70 countries ranked by per capita disability-adjusted life-year (DALY) burden for the three diseases.
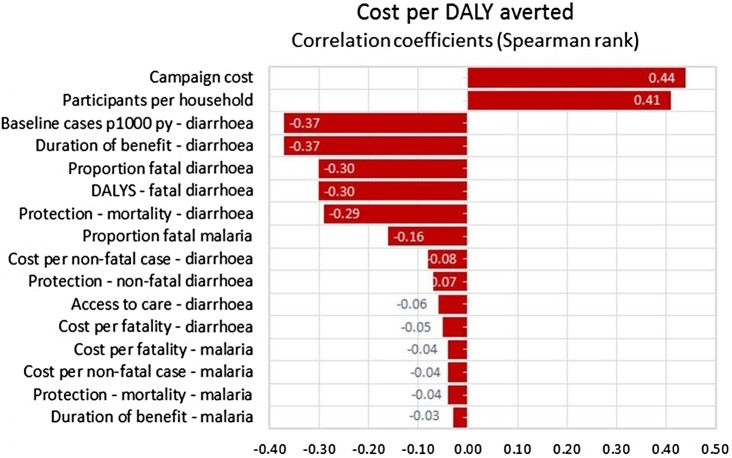
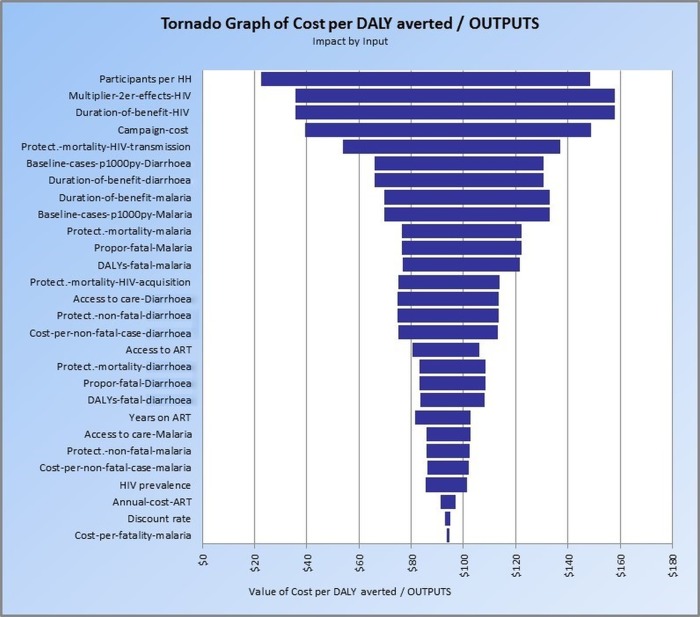
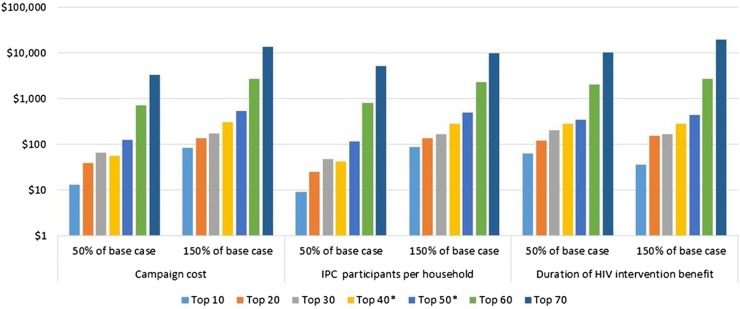
We constructed a deterministic cost-effectiveness model portraying an IPC combining counselling and testing, cotrimoxazole prophylaxis, referral to treatment and condom distribution for HIV prevention; bed nets for malaria prevention; and provision of household water filters for diarrhoea prevention. We developed a mix of empirical and modelled cost and health impact estimates applied to all 70 countries. One-way, multiway and scenario sensitivity analyses were conducted to document the strength of our findings. We used a healthcare payer's perspective, discounted costs and DALYs at 3% per year and denominated cost in 2012 US dollars.
The primary outcome was cost-effectiveness expressed as net cost per DALY averted. Other outcomes included cost of the IPC; net IPC costs adjusted for averted and additional medical costs and DALYs averted.
Implementation of the IPC in the 10 most cost-effective countries at 15% population coverage would cost US$583 million over 3 years (adjusted costs of US$398 million), averting 8.0 million DALYs. Extending IPC programmes to all 70 of the identified high-burden countries at 15% coverage would cost an adjusted US$51.3 billion and avert 78.7 million DALYs. Incremental cost-effectiveness ranged from US$49 per DALY averted for the 10 countries with the most favourable cost-effectiveness to US$119, US$181, US$335, US$1692 and US$8340 per DALY averted as each successive group of 10 countries is added ordered by decreasing cost-effectiveness.
IPC appears cost-effective in many settings, and has the potential to substantially reduce the burden of disease in resource-poor countries. This study increases confidence that IPC can be an important new approach for enhancing global health.
本研究估计了一项综合预防运动(IPC)对70个国家的健康影响、成本及成本效益,这些国家按三种疾病的人均残疾调整生命年(DALY)负担进行排名,该运动聚焦于腹泻、疟疾和艾滋病。
我们构建了一个确定性成本效益模型,描绘了一项IPC,该IPC结合了咨询与检测、复方新诺明预防、转介治疗以及为预防艾滋病发放避孕套;为预防疟疾发放蚊帐;以及为预防腹泻提供家用滤水器。我们制定了一套经验性和模型化的成本及健康影响估计值,并应用于所有70个国家。进行了单向、多向和情景敏感性分析,以证明我们研究结果的可靠性。我们采用医疗保健支付方的视角,按每年3%对成本和DALYs进行贴现,并以2012年美元计价成本。
主要结果是以每避免一个DALY的净成本表示的成本效益。其他结果包括IPC的成本;根据避免和额外的医疗成本以及避免的DALYs调整后的IPC净成本。
在10个最具成本效益的国家实施IPC,覆盖15%的人口,3年内将花费5.83亿美元(调整后成本为3.98亿美元),避免800万个DALY。将IPC项目扩展到所有70个确定的高负担国家,覆盖率为15%,调整后成本将为513亿美元,避免7870万个DALY。增量成本效益从成本效益最有利的10个国家每避免一个DALY的49美元,到按成本效益递减顺序依次增加的每组10个国家每避免一个DALY的119美元、181美元、335美元、1692美元和8340美元不等。
IPC在许多情况下似乎具有成本效益,并且有可能大幅减轻资源匮乏国家的疾病负担。本研究增强了人们对IPC可成为加强全球健康的一种重要新方法的信心。