Department of Health Services, Policy, and Practice, Brown University School of Public Health, 121 South Main Street, Box G-S121-8, Providence, RI, 02912, USA.
Center of Innovation in Long-Term Services and Supports, Providence Veterans Affairs Medical Center, Providence, RI, USA.
Drugs Aging. 2020 Oct;37(10):755-766. doi: 10.1007/s40266-020-00791-w.
Evidence regarding differences in outcomes between angiotensin II receptor blockers (ARBs) and angiotensin-converting enzyme inhibitors (ACEIs) among older nursing home (NH) residents after acute myocardial infarction (AMI) is limited.
The purpose of our study was to estimate the post-AMI effects of ARBs versus ACEIs on mortality, rehospitalization, and functional decline outcomes in this important population.
This retrospective cohort study used national Medicare claims linked to Minimum Data Set assessments. The study population included individuals aged ≥ 65 years who resided in a US NH ≥ 30 days, were hospitalized for AMI between May 2007 and March 2010, and returned to the NH. We compared 90-day mortality, rehospitalization, and functional decline outcomes between ARB and ACEI users with inverse-probability-of-treatment-weighted binomial and multinomial logistic regression models.
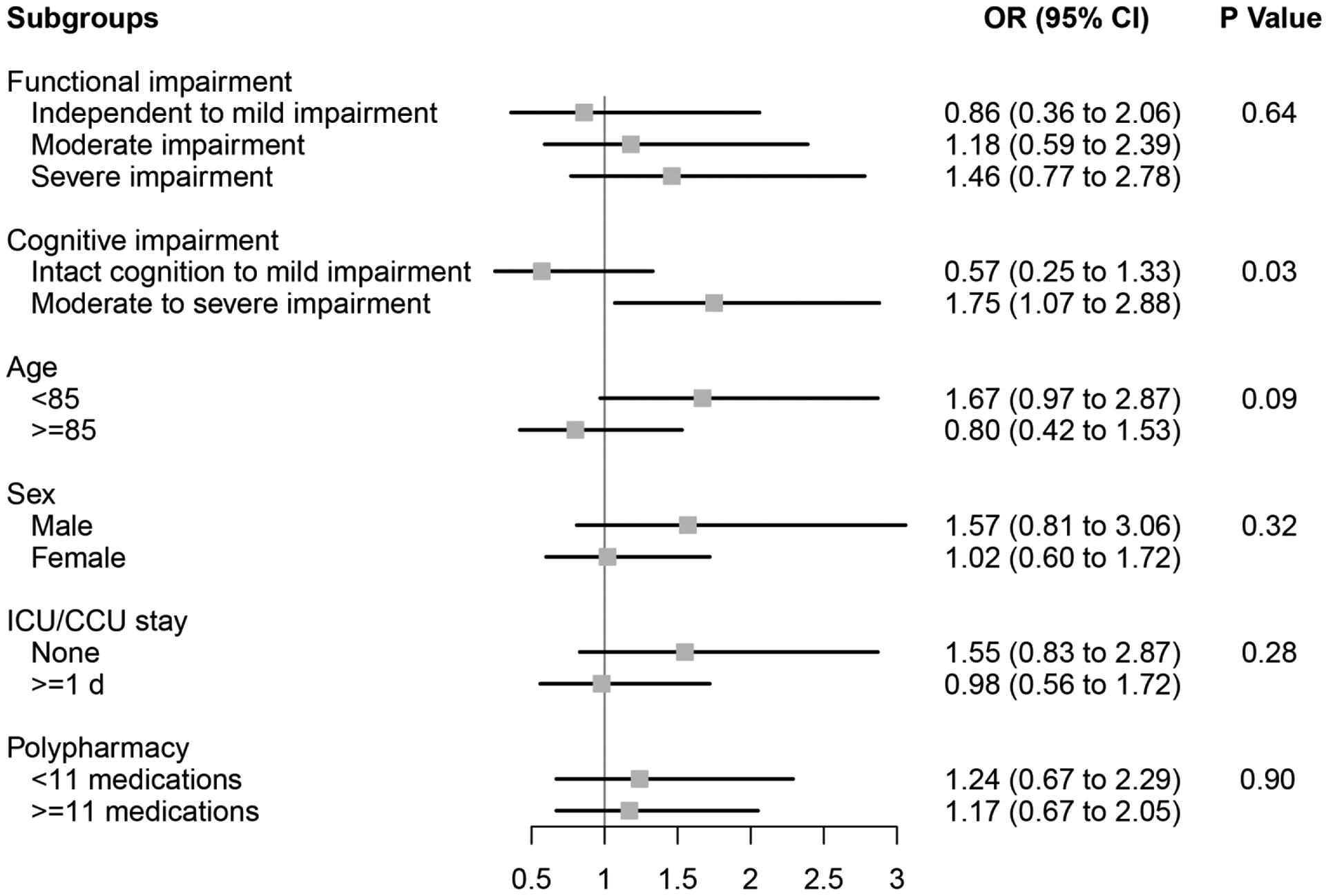
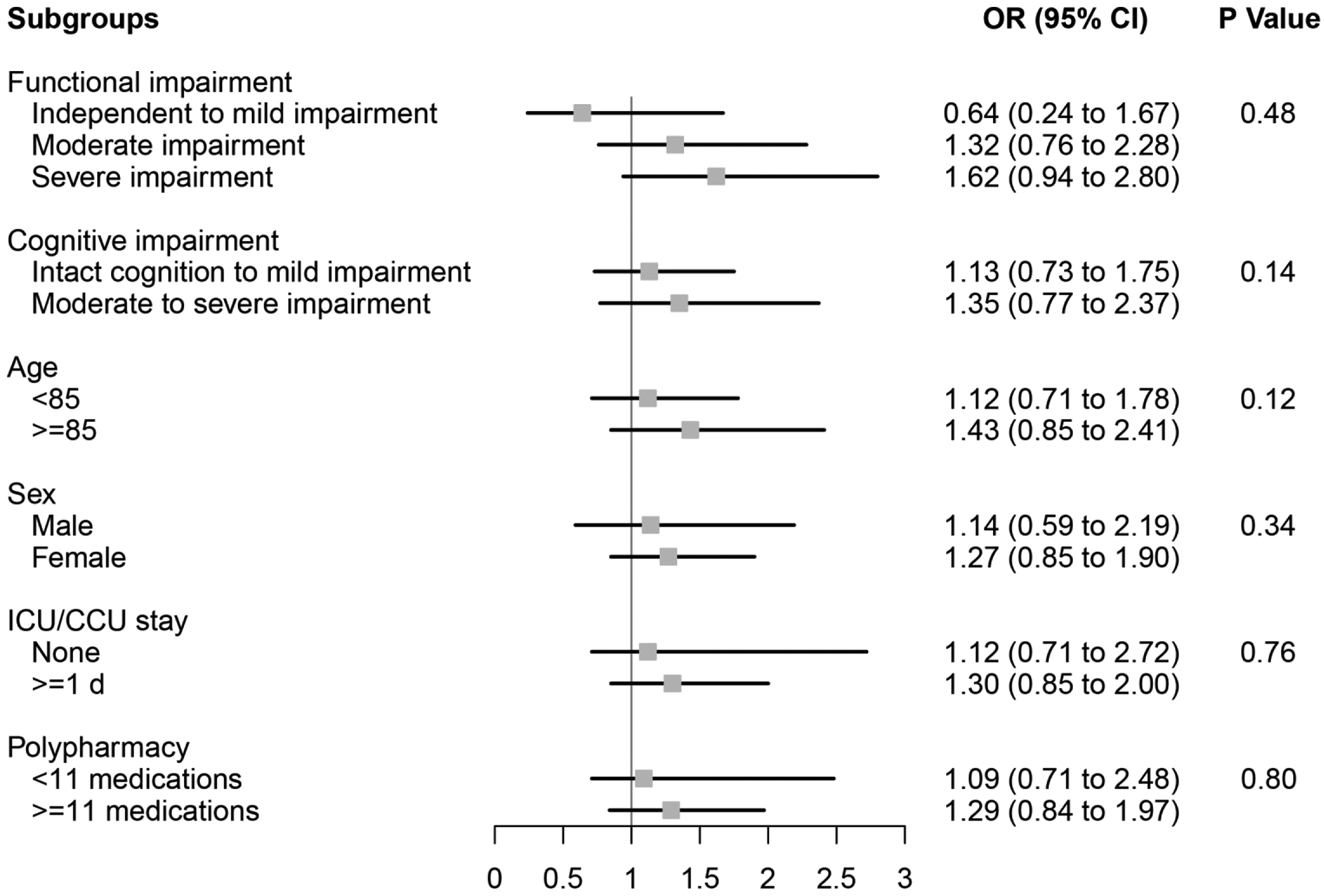
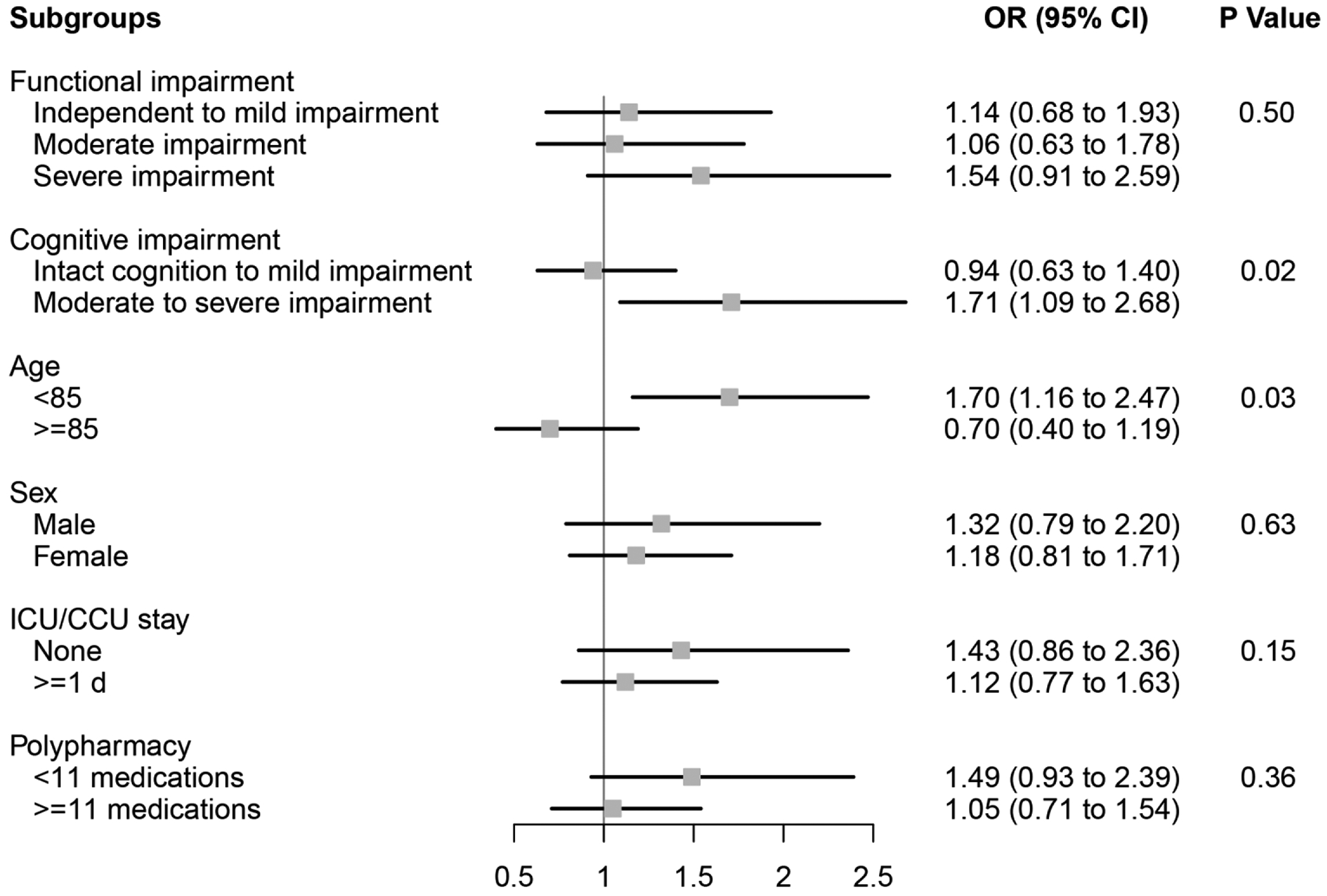
Of the 2765 NH residents, 270 (9.8%) used ARBs and 2495 (90.2%) used ACEIs. The mean age of ARB versus ACEI users was 82.3 versus 82.7 years, respectively. No marked differences existed between ARB and ACEI users for mortality [odds ratio (OR) 1.18; 95% confidence interval (CI) 0.78-1.79], rehospitalization (OR 1.22; 95% CI 0.90-1.65), or functional decline (OR 1.23; 95% CI 0.88-1.74). In subgroup analyses, ARBs were associated with increased mortality and rehospitalization in individuals with moderate to severe cognitive impairment and with increased rehospitalization in those aged < 85 years.
Our findings align with prior data and suggest that clinicians can prescribe either ARBs or ACEIs post-AMI for secondary prevention in NH residents, although the subgroup findings merit further scrutiny and replication. Providers should consider factors such as patient preferences, class-specific adverse events, and costs when prescribing.
关于血管紧张素 II 受体阻滞剂 (ARB) 和血管紧张素转换酶抑制剂 (ACEI) 在急性心肌梗死 (AMI) 后老年疗养院 (NH) 居民之间结局差异的证据有限。
我们的研究目的是评估 ARB 与 ACEI 在该重要人群中对 AMI 后死亡率、再住院和功能下降结局的影响。
这项回顾性队列研究使用了全国性医疗保险索赔与最低数据集评估相关联。研究人群包括年龄≥65 岁、2007 年 5 月至 2010 年 3 月期间因 AMI 住院且在 NH 中至少居住 30 天的个体。我们使用逆概率治疗加权二项式和多项逻辑回归模型比较了 ARB 和 ACEI 使用者的 90 天死亡率、再住院率和功能下降结局。
在 2765 名 NH 居民中,270 名 (9.8%) 使用了 ARB,2495 名 (90.2%) 使用了 ACEI。ARB 使用者和 ACEI 使用者的平均年龄分别为 82.3 岁和 82.7 岁。ARB 使用者和 ACEI 使用者之间的死亡率[比值比 (OR) 1.18;95%置信区间 (CI) 0.78-1.79]、再住院率 (OR 1.22;95% CI 0.90-1.65)或功能下降率 (OR 1.23;95% CI 0.88-1.74)均无显著差异。在亚组分析中,ARB 与中度至重度认知障碍个体的死亡率和再住院率增加以及年龄<85 岁个体的再住院率增加相关。
我们的发现与之前的数据一致,表明临床医生可以在 NH 居民中开具 AMI 后二级预防的 ARB 或 ACEI,尽管亚组结果值得进一步审查和复制。在开处方时,提供者应考虑患者偏好、特定类别不良反应和成本等因素。