Department of Neurosurgery, Nanfang Hospital, Southern Medical University, No. 1838 Guangzhou Avenue North, Guangzhou, 510515, Guangdong, China.
The Laboratory for Precision Neurosurgery, Nanfang Hospital, Southern Medical University, Guangzhou, 510515, Guangdong, China.
BMC Neurol. 2020 Aug 20;20(1):310. doi: 10.1186/s12883-020-01888-w.
Age is associated with the prognosis of glioma patients, but there is no uniform standard of age-group classification to evaluate the prognosis of glioma patients. In this study, we aimed to establish an age group classification for risk stratification in glioma patients.
1502 patients diagnosed with gliomas at Nanfang Hospital between 2000 and 2018 were enrolled. The WHO grade of glioma was used as a dependent variable to evaluate the effect of age on risk stratification. The evaluation model was established by logistic regression, and the Akaike information criterion (AIC) value of the model was used to determine the optimal cutoff points for age-classification. The differences in gender, WHO grade, pathological subtype, tumor cell differentiation, tumor size, tumor location, and molecular markers between different age groups were analyzed. The molecular markers included GFAP, EMA, MGMT, P53, NeuN, Oligo2, EGFR, VEGF, IDH1, Ki-67, PR, CD3, H3K27M, TS, and 1p/19q status.
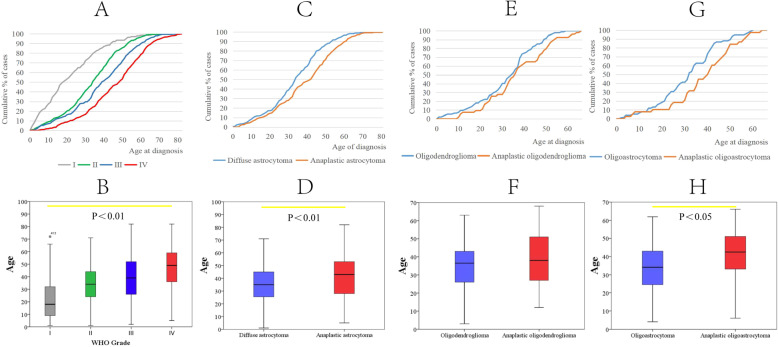
The proportion of men with glioma was higher than that of women with glioma (58.3% vs 41.7%). Analysis of age showed that appropriate classifications of age group were 0-14 years old (pediatric group), 15-47 years old (youth group), 48-63 years old (middle-aged group), and ≥ 64 years old (elderly group).The proportions of glioblastoma and large tumor size (4-6 cm) increased with age (p = 0.000, p = 0.018, respectively). Analysis of the pathological molecular markers across the four age groups showed that the proportion of patients with larger than 10% area of Ki-67 expression or positive PR expression increased with age (p = 0.000, p = 0.017, respectively).
Appropriate classifications of the age group for risk stratification are 0-14 years old (pediatric group), 15-47 years old (young group), 48-63 years old (middle age group) and ≥ 64 years old (elderly group). This age group classification is effective in evaluating the risk of glioblastoma in glioma patients.
年龄与脑胶质瘤患者的预后相关,但目前尚无统一的年龄分组标准来评估脑胶质瘤患者的预后。本研究旨在建立一种年龄分组标准,用于脑胶质瘤患者的风险分层。
纳入 2000 年至 2018 年在南方医院诊断为脑胶质瘤的 1502 例患者。以脑胶质瘤的 WHO 分级为因变量,评估年龄对风险分层的影响。采用逻辑回归建立评估模型,模型的 Akaike 信息准则(AIC)值用于确定年龄分组的最佳截断点。分析不同年龄组患者的性别、WHO 分级、病理亚型、肿瘤细胞分化、肿瘤大小、肿瘤位置和分子标志物的差异。分子标志物包括 GFAP、EMA、MGMT、P53、NeuN、Oligo2、EGFR、VEGF、IDH1、Ki-67、PR、CD3、H3K27M、TS 和 1p/19q 状态。
脑胶质瘤患者中男性比例高于女性(58.3%比 41.7%)。年龄分析显示,年龄分组的合适分类为 0-14 岁(儿童组)、15-47 岁(青年组)、48-63 岁(中年组)和≥64 岁(老年组)。随着年龄的增长,胶质母细胞瘤和较大肿瘤大小(4-6cm)的比例增加(p=0.000,p=0.018)。对四个年龄组的病理分子标志物进行分析显示,Ki-67 表达面积大于 10%或 PR 表达阳性的患者比例随年龄增长而增加(p=0.000,p=0.017)。
用于风险分层的年龄分组的合适分类为 0-14 岁(儿童组)、15-47 岁(青年组)、48-63 岁(中年组)和≥64 岁(老年组)。这种年龄分组标准可有效评估脑胶质瘤患者胶质母细胞瘤的风险。