Loosen Sven H, Schulze-Hagen Maximilian, Püngel Tobias, Bündgens Lukas, Wirtz Theresa, Kather Jakob N, Vucur Mihael, Paffenholz Pia, Demir Münevver, Bruners Philipp, Kuhl Christiane, Trautwein Christian, Tacke Frank, Luedde Tom, Koch Alexander, Roderburg Christoph
Department of Medicine III, University Hospital Rheinisch-Westfälische Technische Hochschule Aachen, Aachen, Germany.
Clinic for Gastroenterology, Hepatology and Infectious Diseases, University Hospital Düsseldorf, Medical Faculty of Heinrich Heine University Düsseldorf, Düsseldorf, Germany.
Crit Care Explor. 2020 Aug 5;2(8):e0171. doi: 10.1097/CCE.0000000000000171. eCollection 2020 Aug.
Parameters of patients' body composition have been suggested as prognostic markers in several clinical conditions including cancer and liver transplantation, but only limited data on its value in critical illness exist to date. In this study, we aimed at evaluating a potential prognostic value of the skeletal muscle mass and skeletal muscle myosteatosis of critically ill patients at admission to the ICU.
Exploratory observational cohort study.
An urban, academic medical institution.
One-hundred fifty-five patients treated for critical illness on a medical ICU.
None.
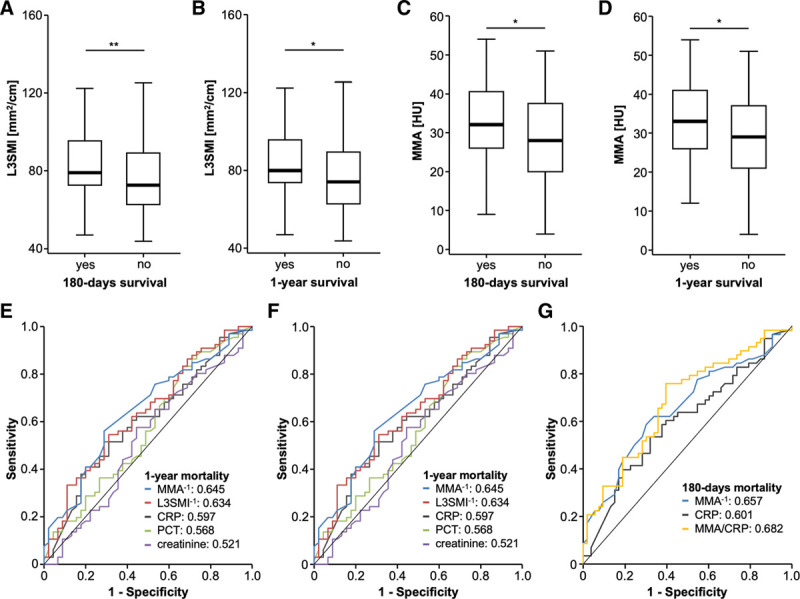
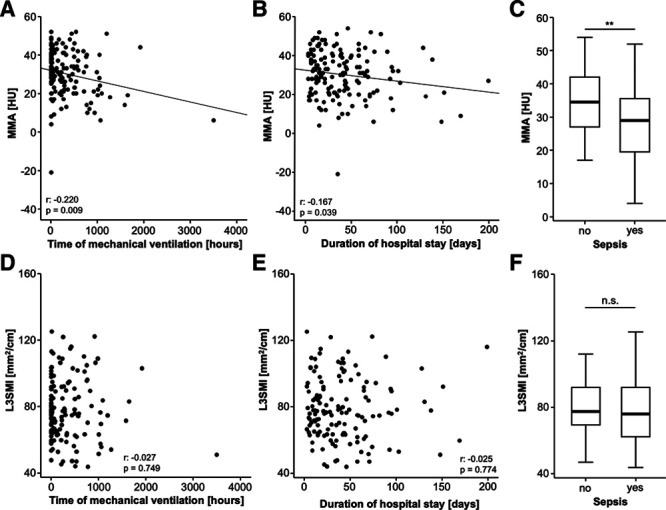
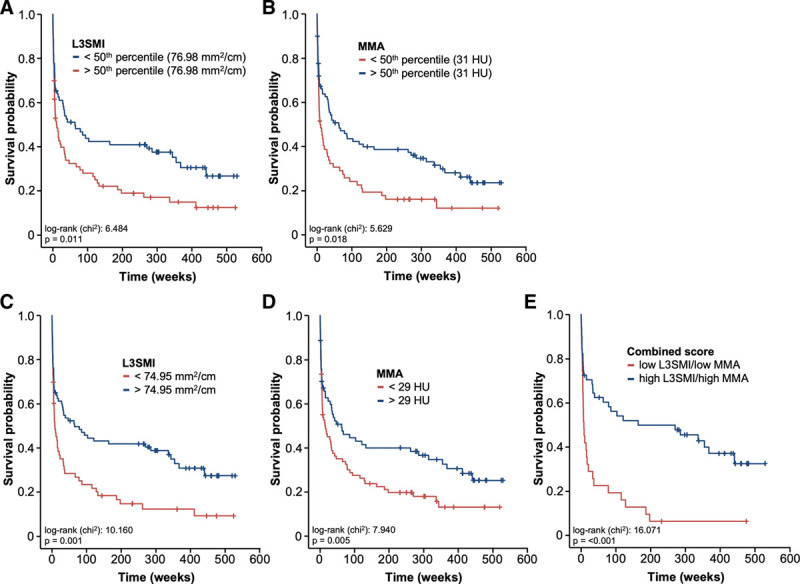
We used routine CT scans to assess the patients' individual body composition. The skeletal muscle index as a surrogate for sarcopenia was defined as the total skeletal muscle area at the level of the third lumbar vertebra on axial CT scan, normalized for the patient's height. Myosteatosis was evaluated by assessing the mean skeletal muscle attenuation measured in Hounsfield unit at the same sectional plane. The skeletal muscle index and mean skeletal muscle attenuation at admission to the ICU were significantly higher in patients with long-term survival (180-day or 1-year mortality), while both parameters were comparable between short-term survivors and nonsurvivors (ICU mortality or 30-d mortality). Patients with a skeletal muscle index or mean skeletal muscle attenuation below our established ideal cutoff values (74.95 mm/cm and 29 Hounsfield unit) showed a significantly reduced overall survival. These findings were confirmed in univariate and multivariate Cox regression analyses. Furthermore, myosteatosis significantly correlated with the time of mechanical ventilation, the duration of hospital stay, and the presence of sepsis.
Our data suggest that sarcopenia and myosteatosis represent important prognostic factors in critically ill patients that can be easily obtained from routine CT scans. Both parameters at admission to the ICU yield important information on the patients' long-term outcome and might be used for early clinical decision-making in these patients.
在包括癌症和肝移植在内的多种临床情况下,患者身体成分参数已被提议作为预后标志物,但迄今为止,关于其在危重症中的价值仅有有限的数据。在本研究中,我们旨在评估重症监护病房(ICU)入院时危重症患者骨骼肌质量和骨骼肌肌脂肪变性的潜在预后价值。
探索性观察性队列研究。
一家城市学术医疗机构。
155例在医疗ICU接受危重症治疗的患者。
无。
我们使用常规CT扫描评估患者的个体身体成分。作为肌肉减少症替代指标的骨骼肌指数定义为轴向CT扫描第三腰椎水平的总骨骼肌面积,并根据患者身高进行标准化。通过评估在同一截面平面上以亨氏单位测量的平均骨骼肌衰减来评估肌脂肪变性。长期存活(180天或1年死亡率)患者在ICU入院时的骨骼肌指数和平均骨骼肌衰减显著更高,而短期存活者和非存活者(ICU死亡率或30天死亡率)之间这两个参数相当。骨骼肌指数或平均骨骼肌衰减低于我们确定的理想临界值(74.95 mm/cm和29亨氏单位)的患者总体生存率显著降低。这些发现在单因素和多因素Cox回归分析中得到证实。此外,肌脂肪变性与机械通气时间、住院时间和脓毒症的存在显著相关。
我们的数据表明,肌肉减少症和肌脂肪变性是危重症患者的重要预后因素,可通过常规CT扫描轻松获得。ICU入院时的这两个参数都能提供有关患者长期预后的重要信息,并可能用于这些患者的早期临床决策。