Department of Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario, Canada; Department of Medicine, McMaster University, Hamilton, Ontario, Canada; Hamilton Regional Laboratory Medicine Program (Transfusion Medicine), Hamilton, Ontario, Canada; Service of Clinical Hematology, Hamilton Health Sciences (Hamilton General Hospital), Canada.
Division of Hospital Medicine, Henry Ford Hospital, Detroit, MI, United States of America.
Thromb Res. 2020 Dec;196:38-51. doi: 10.1016/j.thromres.2020.08.017. Epub 2020 Aug 10.
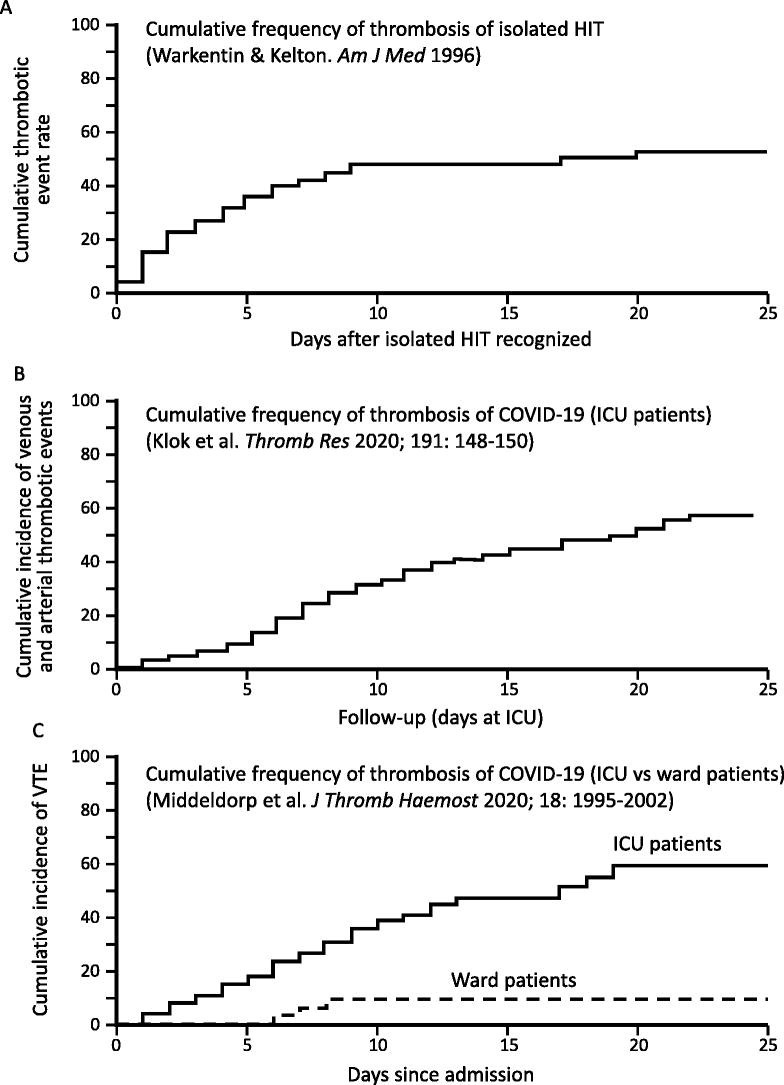
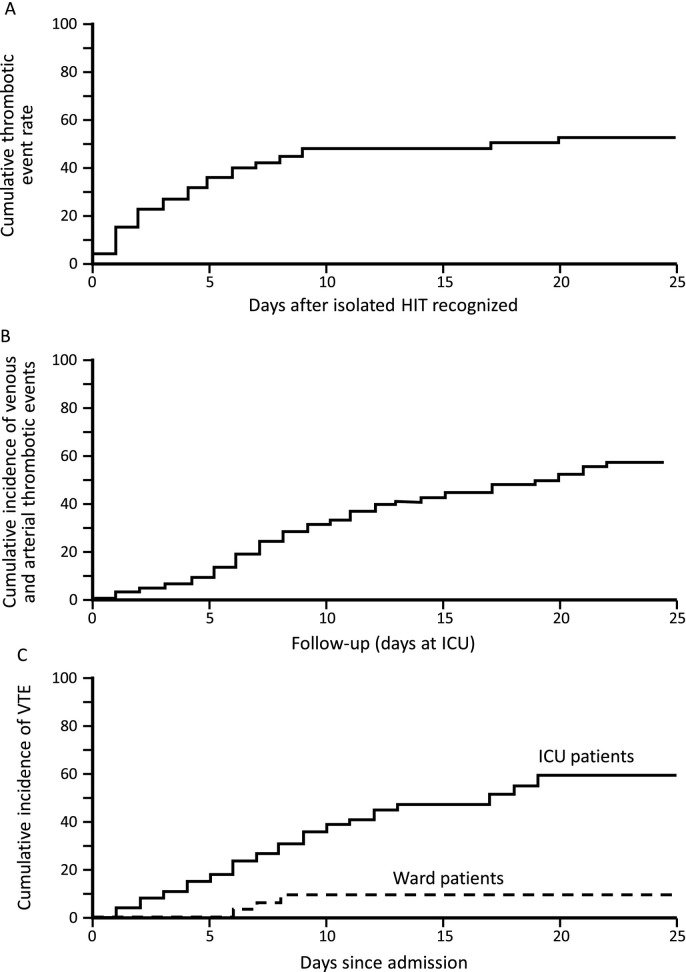
A striking feature of COVID-19 is the high frequency of thrombosis, particularly in patients who require admission to intensive care unit because of respiratory complications (pneumonia/adult respiratory distress syndrome). The spectrum of thrombotic events is wide, including in situ pulmonary thrombosis, deep-vein thrombosis and associated pulmonary embolism, as well as arterial thrombotic events (stroke, myocardial infarction, limb artery thrombosis). Unusual thrombotic events have also been reported, e.g., cerebral venous sinus thrombosis, mesenteric artery and vein thrombosis. Several hematology abnormalities have been observed in COVID-19 patients, including lymphopenia, neutrophilia, thrombocytopenia (usually mild), thrombocytosis, elevated prothrombin time and partial thromboplastin times (the latter abnormality often indicating lupus anticoagulant phenomenon), hyperfibrinogenemia, elevated von Willebrand factor levels, and elevated fibrin d-dimer. Many of these abnormal hematologic parameters-even as early as the time of initial hospital admission-indicate adverse prognosis, including greater frequency of progression to severe respiratory illness and death. Progression to overt disseminated intravascular coagulation in fatal COVID-19 has been reported in some studies, but not observed in others. We compare and contrast COVID-19 hypercoagulability, and associated increased risk of venous and arterial thrombosis, from the perspective of heparin-induced thrombocytopenia (HIT), including the dilemma of providing thromboprophylaxis and treatment recommendations when available data are limited to observational studies. The frequent use of heparin-both low-molecular-weight and unfractionated-in preventing and treating COVID-19 thrombosis, means that vigilance for HIT occurrence is required in this patient population.
COVID-19 的一个显著特征是血栓形成的频率很高,尤其是在因呼吸并发症(肺炎/成人呼吸窘迫综合征)需要入住重症监护病房的患者中。血栓形成事件的范围很广,包括原位肺血栓形成、深静脉血栓形成和相关的肺栓塞,以及动脉血栓形成事件(中风、心肌梗死、肢体动脉血栓形成)。也有报道称发生了不常见的血栓形成事件,例如脑静脉窦血栓形成、肠系膜动脉和静脉血栓形成。COVID-19 患者观察到几种血液学异常,包括淋巴细胞减少、中性粒细胞增多、血小板减少症(通常为轻度)、血小板增多症、凝血酶原时间和部分凝血活酶时间升高(后者异常通常提示狼疮抗凝物现象)、纤维蛋白原血症、血管性血友病因子水平升高和纤维蛋白 D-二聚体升高。这些异常的血液学参数中的许多参数——甚至早在最初住院时就已经出现——表明预后不良,包括更频繁地进展为严重呼吸疾病和死亡。一些研究报道了致命 COVID-19 中显性弥散性血管内凝血的进展,但其他研究并未观察到。我们从肝素诱导的血小板减少症(HIT)的角度比较和对比 COVID-19 的高凝状态以及与之相关的静脉和动脉血栓形成风险增加,包括在可用数据仅限于观察性研究的情况下提供血栓预防和治疗建议时所面临的困境。肝素(包括低分子量肝素和未分级肝素)在预防和治疗 COVID-19 血栓形成中的频繁使用意味着在这一患者人群中需要警惕 HIT 的发生。