Department of Cellular Pathology, Northwest London Pathology, Imperial College London NHS Trust, London, UK.
Centre for Haematology, Faculty of Medicine, Imperial College London, London, UK.
Lancet Microbe. 2020 Oct;1(6):e245-e253. doi: 10.1016/S2666-5247(20)30115-4. Epub 2020 Aug 20.
Severe COVID-19 has a high mortality rate. Comprehensive pathological descriptions of COVID-19 are scarce and limited in scope. We aimed to describe the histopathological findings and viral tropism in patients who died of severe COVID-19.
In this case series, patients were considered eligible if they were older than 18 years, with premortem diagnosis of severe acute respiratory syndrome coronavirus 2 infection and COVID-19 listed clinically as the direct cause of death. Between March 1 and April 30, 2020, full post-mortem examinations were done on nine patients with confirmed COVID-19, including sampling of all major organs. A limited autopsy was done on one additional patient. Histochemical and immunohistochemical analyses were done, and histopathological findings were reported by subspecialist pathologists. Viral quantitative RT-PCR analysis was done on tissue samples from a subset of patients.
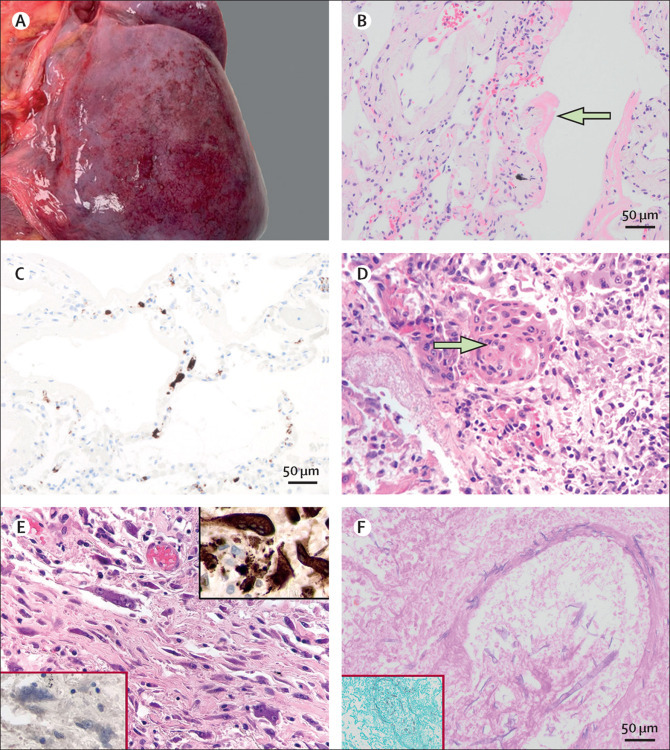
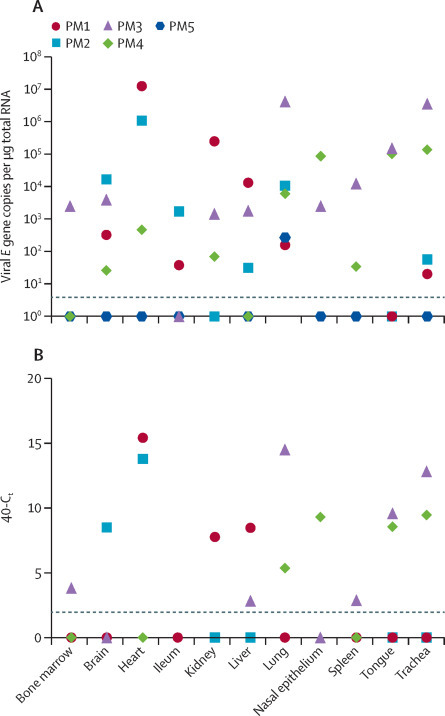
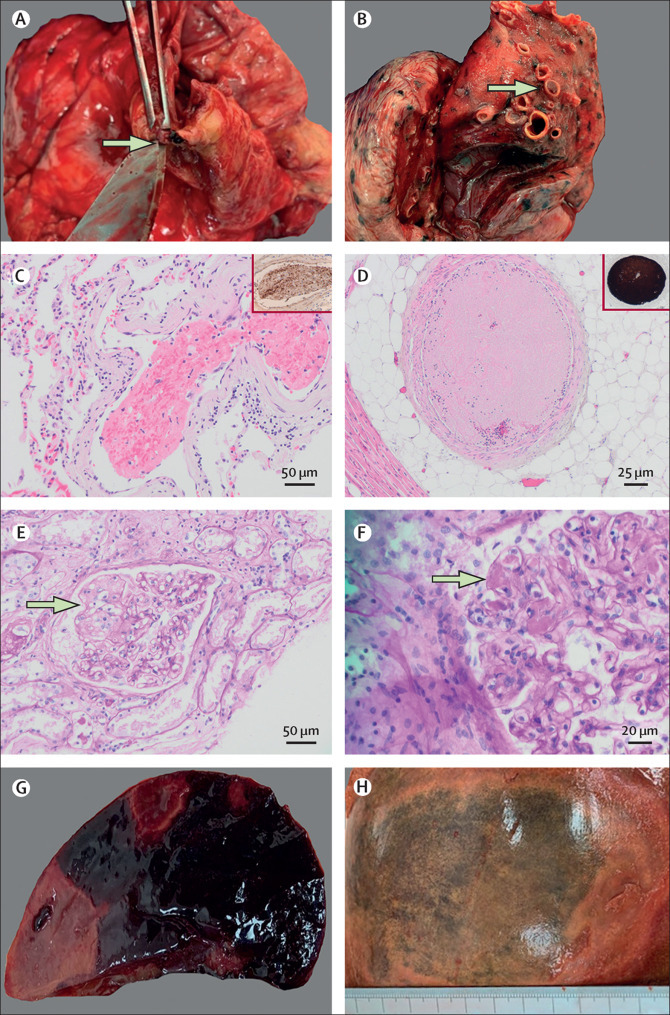
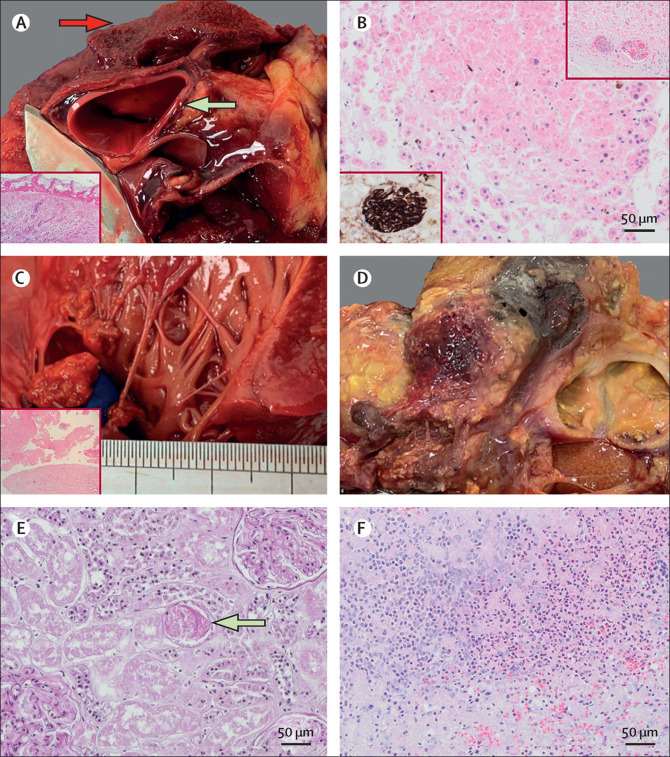
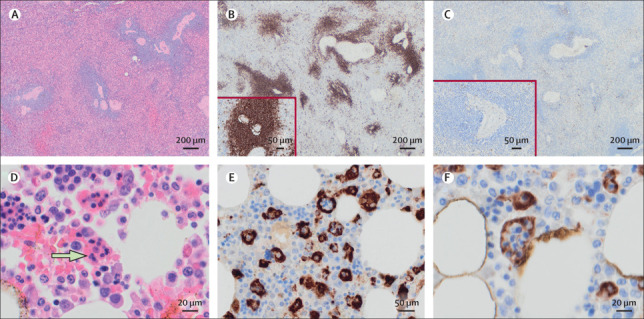
The median age at death of our cohort of ten patients was 73 years (IQR 52-79). Thrombotic features were observed in at least one major organ in all full autopsies, predominantly in the lung (eight [89%] of nine patients), heart (five [56%]), and kidney (four [44%]). Diffuse alveolar damage was the most consistent lung finding (all ten patients); however, organisation was noted in patients with a longer clinical course. We documented lymphocyte depletion (particularly CD8-positive T cells) in haematological organs and haemophagocytosis. Evidence of acute tubular injury was noted in all nine patients examined. Major unexpected findings were acute pancreatitis (two [22%] of nine patients), adrenal micro-infarction (three [33%]), pericarditis (two [22%]), disseminated mucormycosis (one [10%] of ten patients), aortic dissection (one [11%] of nine patients), and marantic endocarditis (one [11%]). Viral genomes were detected outside of the respiratory tract in four of five patients. The presence of subgenomic viral RNA transcripts provided evidence of active viral replication outside the respiratory tract in three of five patients.
Our series supports clinical data showing that the four dominant interrelated pathological processes in severe COVID-19 are diffuse alveolar damage, thrombosis, haemophagocytosis, and immune cell depletion. Additionally, we report here several novel autopsy findings including pancreatitis, pericarditis, adrenal micro-infarction, secondary disseminated mucormycosis, and brain microglial activation, which require additional investigation to understand their role in COVID-19.
Imperial Biomedical Research Centre, Wellcome Trust, Biotechnology and Biological Sciences Research Council.
严重的 COVID-19 死亡率很高。目前对 COVID-19 的全面病理描述很少且范围有限。我们旨在描述死于严重 COVID-19 的患者的组织病理学发现和病毒嗜性。
在本病例系列研究中,患者如果年龄大于 18 岁,且生前诊断为严重急性呼吸综合征冠状病毒 2 感染和 COVID-19,且临床上将 COVID-19 列为直接死亡原因,则被认为符合条件。2020 年 3 月 1 日至 4 月 30 日,对 9 名确诊 COVID-19 的患者进行了全面的尸检,包括对所有主要器官进行取样。对另外 1 名患者进行了有限的解剖。进行了组织化学和免疫组织化学分析,并由专科病理学家报告了组织病理学发现。对部分患者的组织样本进行了病毒定量 RT-PCR 分析。
我们的十名患者队列的中位死亡年龄为 73 岁(IQR 52-79)。所有全尸检均至少在一个主要器官中观察到血栓特征,主要在肺(9 名患者中的 8 名[89%])、心脏(5 名[56%])和肾脏(4 名[44%])。弥漫性肺泡损伤是最常见的肺部发现(所有十名患者);然而,在临床病程较长的患者中观察到了组织形成。我们记录了血液系统器官中淋巴细胞耗竭(尤其是 CD8 阳性 T 细胞)和噬血细胞现象。所有检查的 9 名患者均有急性肾小管损伤的证据。在 9 名患者中的 2 名(22%)中发现了急性胰腺炎,在 3 名(33%)中发现了肾上腺微梗死,在 2 名(22%)中发现了心包炎,在 10 名患者中的 1 名(10%)中发现了播散性毛霉菌病,在 9 名患者中的 1 名(11%)中发现了主动脉夹层,在 1 名(11%)中发现了心内膜炎。在 5 名患者中的 4 名中,在呼吸道外检测到了病毒基因组。呼吸道外亚基因组病毒 RNA 转录本的存在提供了证据,表明呼吸道外存在活跃的病毒复制。
我们的系列研究支持临床数据,表明严重 COVID-19 的四个主要相互关联的病理过程是弥漫性肺泡损伤、血栓形成、噬血细胞现象和免疫细胞耗竭。此外,我们在此报告了一些新的尸检发现,包括胰腺炎、心包炎、肾上腺微梗死、继发播散性毛霉菌病和大脑小胶质细胞激活,这些发现需要进一步研究以了解它们在 COVID-19 中的作用。
帝国生物医学研究中心、惠康信托基金会、生物技术和生物科学研究理事会。