Department of Radiology, Graduate School of Medical Science, University of the Ryukyus, 207 Uehara, Nishihara, Okinawa, 903-0215, Japan.
Radiation Therapy Center, Okinawa Chubu Hospital, 281 Miyazato, Uruma, Okinawa, 904-2293, Japan.
Int J Clin Oncol. 2020 Nov;25(11):1977-1984. doi: 10.1007/s10147-020-01736-4. Epub 2020 Aug 27.
This prospective study investigated the feasibility, toxicity, and oncologic outcomes of definitive radiotherapy (RT) consisting of whole pelvic radiotherapy with no central shielding (noCS-WPRT) and CT-based intracavitary brachytherapy (ICBT) in Japanese patients with cervical cancer.
Patients with cervical cancer of FIGO stages IB1-IVA were eligible. The treatment protocol consisted of noCS-WPRT of 45 Gy in 25 fractions and CT-based high dose-rate ICBT of 15 or 20 Gy in 3 or 4 fractions prescribed at point A. The prescribed ICBT dose was decreased if the manual dwell time/position optimization failed to meet organs-at-risk constraints. Graphical optimization and additional interstitial needles were not applied.
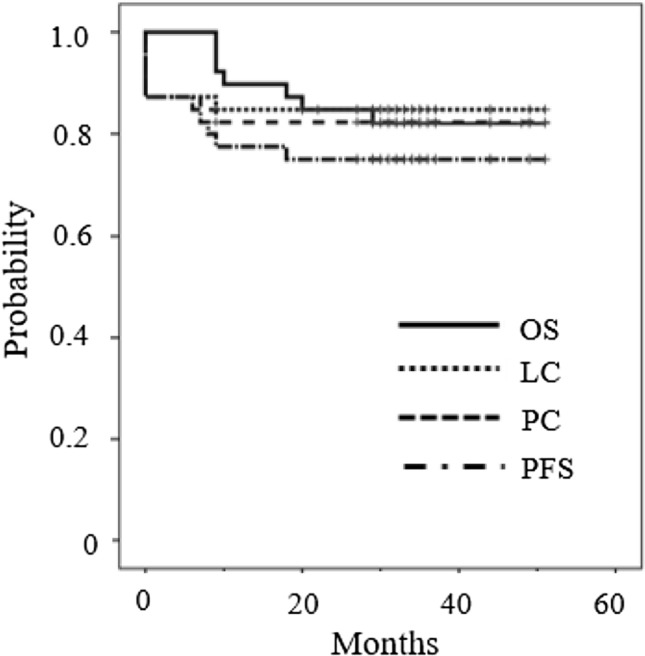
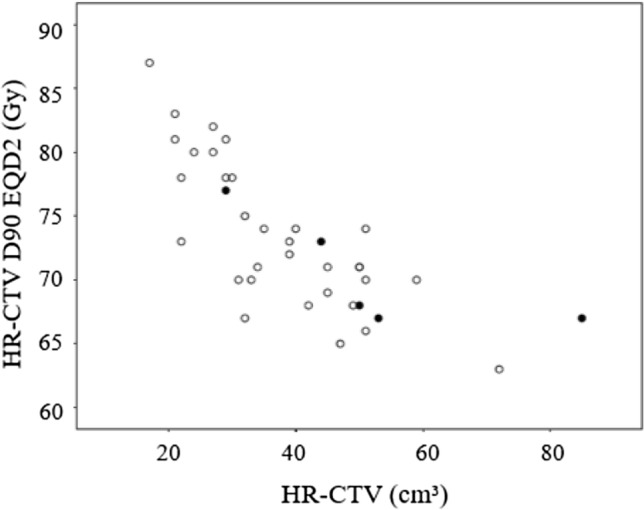
We enrolled 40 patients. FIGO stages were IB1: 11, IB2: 13, IIA2: 1, IIB: 11, IIIB: 3, and IVA: 1. Median (range) pretreatment tumor diameter was 47 (14-81) mm. Point A doses were decreased in 19 of 153 ICBT sessions (12%). The median follow-up duration was 33 months. The 2-year rates of pelvic control, local control (LC), and progression-free survival were 83%, 85%, and 75%, respectively. Pre-ICBT tumor diameter, high-risk clinical target volume (HR-CTV), total HR-CTV D90, and overall treatment time (OTT) significantly affected LC. Late adverse events (grade ≥ 3) were observed in 3 patients (2 in the bladder, 1 in the rectum).
Definitive RT consisting of noCS-WPRT and CT-based ICBT was feasible for Japanese patients with cervical cancer. To further improve LC, additional interstitial needles for patients with a large HR-CTV and shorter OTT should be considered.
本前瞻性研究调查了日本宫颈癌患者接受全盆腔放疗(noCS-WPRT)联合 CT 引导腔内近距离放疗(ICBT)的可行性、毒性和肿瘤学结果。
纳入FIGO 分期为 IB1-IVA 的宫颈癌患者。治疗方案包括 45Gy/25 次的全盆腔无中央屏蔽放疗(noCS-WPRT)和 CT 引导的高剂量率腔内放疗(ICBT),A 点处方剂量为 15 或 20Gy,共 3 或 4 次。如果手动驻留时间/位置优化无法满足危及器官的限制,则降低处方 ICBT 剂量。未应用图形优化和额外的间质针。
共纳入 40 例患者。FIGO 分期为 IB1 期 11 例、IB2 期 13 例、IIA2 期 1 例、IIB 期 11 例、IIIB 期 3 例和 IVA 期 1 例。治疗前肿瘤直径中位数(范围)为 47(14-81)mm。153 次 ICBT 治疗中有 19 次(12%)降低了 A 点剂量。中位随访时间为 33 个月。盆腔控制、局部控制(LC)和无进展生存的 2 年率分别为 83%、85%和 75%。ICBT 前肿瘤直径、高危临床靶区(HR-CTV)、总 HR-CTV D90 和总治疗时间(OTT)显著影响 LC。3 例(2 例膀胱、1 例直肠)发生 3 级及以上晚期不良反应。
对于日本宫颈癌患者,全盆腔无中央屏蔽放疗(noCS-WPRT)联合 CT 引导腔内近距离放疗(ICBT)的根治性放疗是可行的。为了进一步提高 LC,对于 HR-CTV 较大和 OTT 较短的患者,应考虑增加间质针。