Department of Public Health, Erasmus University Medical Center, Rotterdam, the Netherlands.
Departments of Family and Social Medicine and Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, NY, USA.
J Natl Cancer Inst. 2021 Apr 6;113(4):434-442. doi: 10.1093/jnci/djaa127.
We assessed the clinical utility of a first-degree breast cancer family history and polygenic risk score (PRS) to inform screening decisions among women aged 30-50 years.
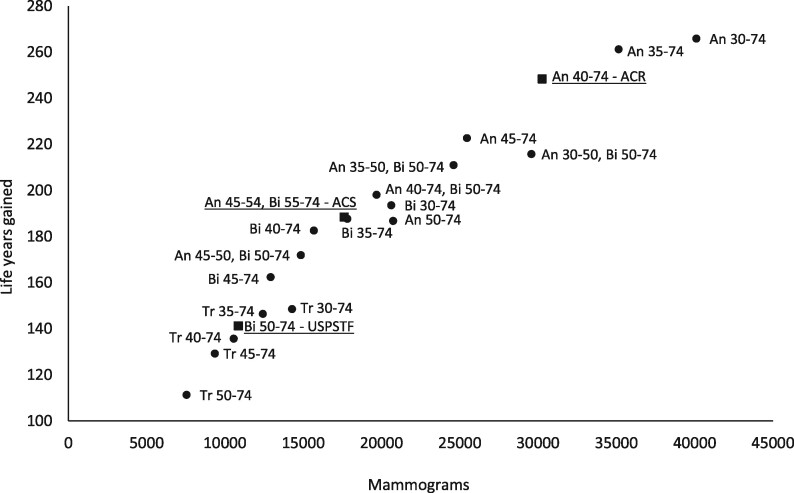
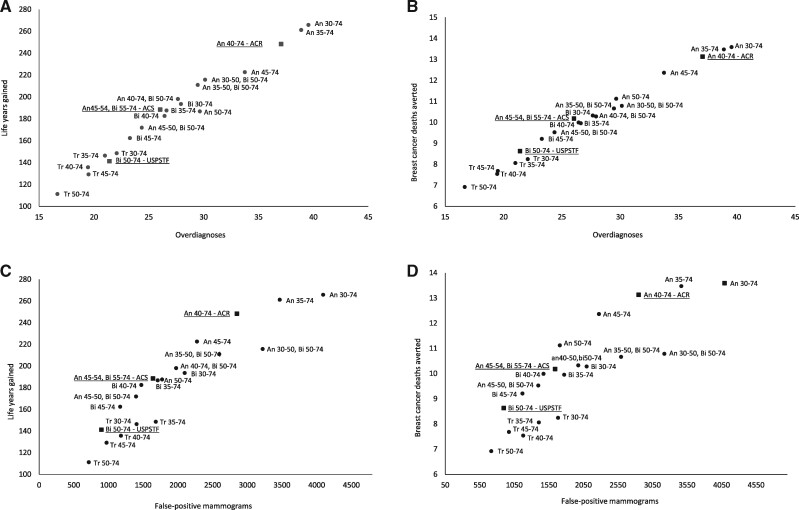
Two established breast cancer models evaluated digital mammography screening strategies in the 1985 US birth cohort by risk groups defined by family history and PRS based on 313 single nucleotide polymorphisms. Strategies varied in initiation age (30, 35, 40, 45, and 50 years) and interval (annual, hybrid, biennial, triennial). The benefits (breast cancer deaths averted, life-years gained) and harms (false-positive mammograms, overdiagnoses) were compared with those seen with 3 established screening guidelines.
Women with a breast cancer family history who initiated biennial screening at age 40 years (vs 50 years) had a 36% (model range = 29%-40%) increase in life-years gained and 20% (model range = 16%-24%) more breast cancer deaths averted, but 21% (model range = 17%-23%) more overdiagnoses and 63% (model range = 62%-64%) more false positives. Screening tailored to PRS vs biennial screening from 50 to 74 years had smaller positive effects on life-years gained (20%) and breast cancer deaths averted (11%) but also smaller increases in overdiagnoses (10%) and false positives (26%). Combined use of family history and PRS vs biennial screening from 50 to 74 years had the greatest increase in life-years gained (29%) and breast cancer deaths averted (18%).
Our results suggest that breast cancer family history and PRS could guide screening decisions before age 50 years among women at increased risk for breast cancer but expected increases in overdiagnoses and false positives should be expected.
我们评估了一级乳腺癌家族史和多基因风险评分(PRS)在指导 30-50 岁女性筛查决策方面的临床实用性。
两个已建立的乳腺癌模型通过基于 313 个单核苷酸多态性的家族史和 PRS 定义的风险组评估了数字乳腺摄影筛查策略,这些策略适用于 1985 年美国出生队列。策略在起始年龄(30、35、40、45 和 50 岁)和间隔(年度、混合、每两年、每三年)上有所不同。与 3 种已建立的筛查指南相比,比较了这些策略的获益(乳腺癌死亡人数减少、生命年增加)和危害(假阳性乳房 X 光片、过度诊断)。
与 50 岁开始每两年筛查相比,具有乳腺癌家族史的女性在 40 岁开始每两年筛查(vs 50 岁),生命年增加 36%(模型范围为 29%-40%),乳腺癌死亡人数减少 20%(模型范围为 16%-24%),但过度诊断增加 21%(模型范围为 17%-23%),假阳性增加 63%(模型范围为 62%-64%)。与从 50 岁至 74 岁的每两年筛查相比,针对 PRS 的筛查更倾向于生命年增加(20%)和乳腺癌死亡人数减少(11%),但过度诊断增加(10%)和假阳性增加(26%)也较小。与从 50 岁至 74 岁的每两年筛查相比,家族史和 PRS 的联合使用在生命年增加(29%)和乳腺癌死亡人数减少(18%)方面有最大的增加。
我们的结果表明,乳腺癌家族史和 PRS 可以在增加乳腺癌风险的女性 50 岁之前指导筛查决策,但预计过度诊断和假阳性的增加是不可避免的。