Structural Heart and Valve Center Vanderbilt University Medical Center Nashville TN.
Cardiovascular Medicine Division Vanderbilt University Medical Center Nashville TN.
J Am Heart Assoc. 2020 Sep;9(17):e017075. doi: 10.1161/JAHA.120.017075. Epub 2020 Aug 28.
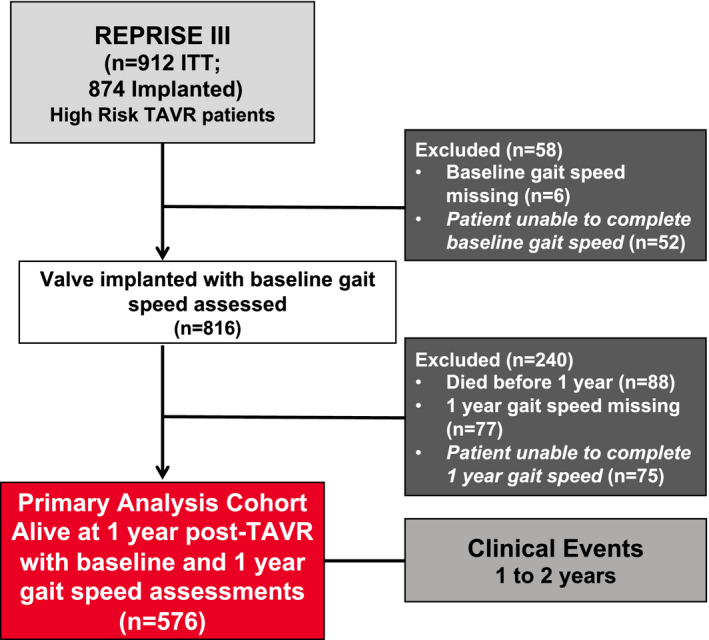
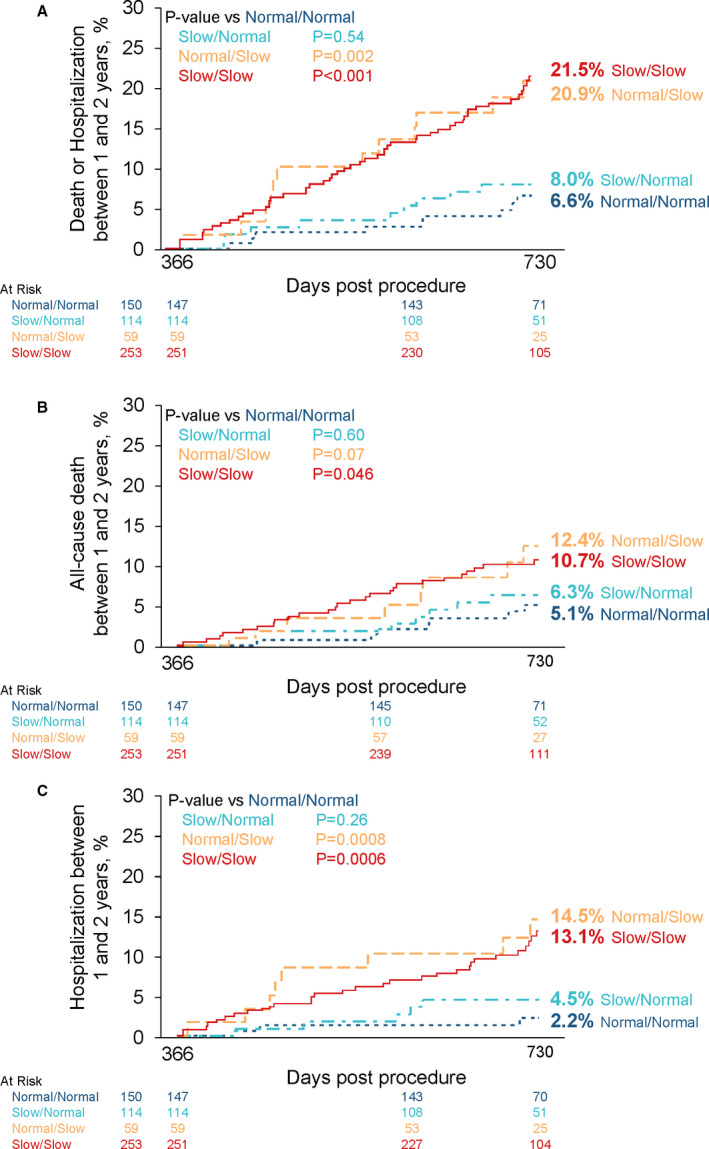
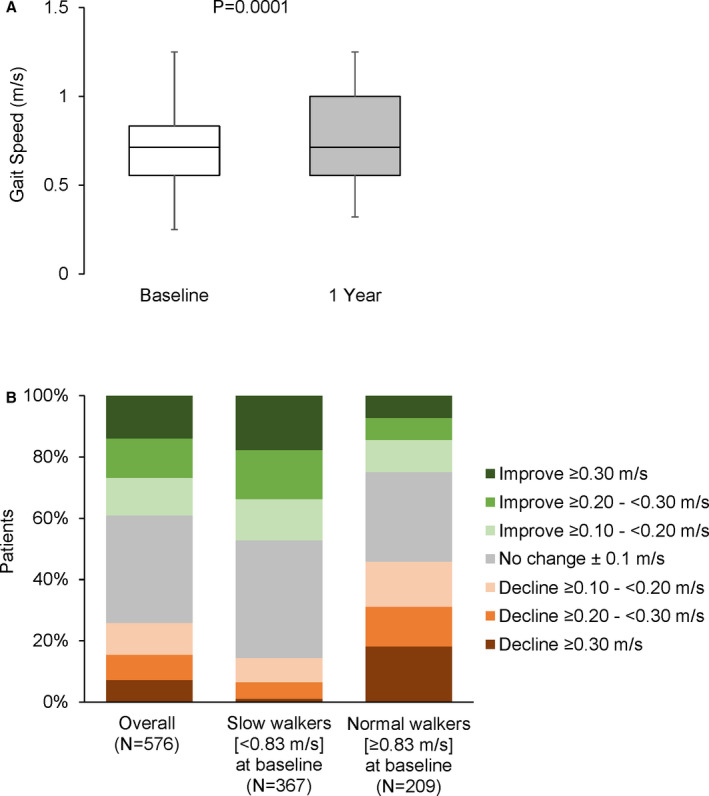
Background Gait speed is a reliable measure of physical function and frailty in patients with aortic stenosis undergoing transcatheter aortic valve replacement (TAVR). Slow gait speed pre-TAVR predicts worse clinical outcomes post-TAVR. The consequences of improved versus worsened physical function post-TAVR are unknown. Methods and Results The REPRISE III (Repositionable Percutaneous Replacement of Stenotic Aortic Valve Through Implantation of Lotus Valve System-Randomized Clinical Evaluation) trial randomized high/extreme risk patients to receive a mechanically-expanded or self-expanding transcatheter heart valve. Of 874 patients who underwent TAVR, 576 with complete data at baseline and 1 year were included in this analysis. Slow gait speed in the 5-m walk test was defined as <0.83 m/s. A clinically meaningful improvement (≥0.1 m/s) in gait speed 1 year after TAVR occurred in 39% of patients, 35% exhibited no change, and 26% declined (≥0.1 m/s). Among groups defined by baseline/1-year post-TAVR gait speeds, 1- to 2-year mortality or hospitalization rates were as follows: 6.6% (normal/normal), 8.0% (slow/normal), 20.9% (normal/slow), and 21.5% (slow/slow). After adjustment, slow gait speed at 1 year (regardless of baseline speed) was associated with a 3.5-fold increase in death/hospitalization between 1 and 2 years compared with those with normal baseline/1-year gait speed. Patients whose slow gait speed normalized at 1 year had no increased risk. One-year, but not baseline, gait speed was associated with death or hospitalization between 1 and 2 years (adjusted hazard ratio, 0.83 per 0.1 m/s faster gait; 95% CI, 0.74-0.93, =0.001). Conclusions Marked heterogeneity exists in the trajectory of physical function after TAVR and this, more than baseline function, has clinical consequences. Identifying and optimizing factors associated with physical resilience after TAVR may improve outcomes. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02202434.
在接受经导管主动脉瓣置换术(TAVR)的主动脉瓣狭窄患者中,步速是身体功能和虚弱的可靠衡量标准。TAVR 前步速较慢预示着 TAVR 后临床结局较差。TAVR 后身体功能改善与恶化的后果尚不清楚。
REPRISE III(通过植入 Lotus 瓣膜系统经皮置换狭窄主动脉瓣的可重新定位的经皮置换-随机临床评估)试验将高危/极高危患者随机分为接受机械扩张或自扩张经导管心脏瓣膜治疗。在接受 TAVR 的 874 例患者中,有 576 例患者在基线和 1 年时具有完整数据,纳入本分析。5 米步行测试中步速较慢定义为<0.83 m/s。TAVR 后 1 年,39%的患者步速有临床意义的改善(≥0.1 m/s),35%无变化,26%下降(≥0.1 m/s)。根据基线/1 年后 TAVR 步速分组,1 至 2 年死亡率或住院率如下:6.6%(正常/正常)、8.0%(缓慢/正常)、20.9%(正常/缓慢)和 21.5%(缓慢/缓慢)。校正后,1 年时步速缓慢(无论基线速度如何)与 1 至 2 年内死亡/住院风险增加 3.5 倍相关,与基线/1 年步速正常的患者相比。1 年内步速缓慢恢复正常的患者无增加的风险。1 年时的步速,而不是基线时的步速,与 1 至 2 年内的死亡或住院相关(校正后的危险比,每 0.1 m/s 更快的步速增加 0.83;95%CI,0.74-0.93,=0.001)。
TAVR 后身体功能的轨迹存在明显的异质性,而且这比基线功能更具有临床意义。确定和优化 TAVR 后身体恢复力相关的因素可能改善结局。