Lemieux Jacob E, Siddle Katherine J, Shaw Bennett M, Loreth Christine, Schaffner Stephen F, Gladden-Young Adrianne, Adams Gordon, Fink Timelia, Tomkins-Tinch Christopher H, Krasilnikova Lydia A, DeRuff Katherine C, Rudy Melissa, Bauer Matthew R, Lagerborg Kim A, Normandin Erica, Chapman Sinead B, Reilly Steven K, Anahtar Melis N, Lin Aaron E, Carter Amber, Myhrvold Cameron, Kemball Molly E, Chaluvadi Sushma, Cusick Caroline, Flowers Katelyn, Neumann Anna, Cerrato Felecia, Farhat Maha, Slater Damien, Harris Jason B, Branda John, Hooper David, Gaeta Jessie M, Baggett Travis P, O'Connell James, Gnirke Andreas, Lieberman Tami D, Philippakis Anthony, Burns Meagan, Brown Catherine M, Luban Jeremy, Ryan Edward T, Turbett Sarah E, LaRocque Regina C, Hanage William P, Gallagher Glen R, Madoff Lawrence C, Smole Sandra, Pierce Virginia M, Rosenberg Eric, Sabeti Pardis C, Park Daniel J, Maclnnis Bronwyn L
Broad Institute of Harvard and MIT, 75 Ames Street, Cambridge, MA 02142, USA.
Division of Infectious Diseases, Massachusetts General Hospital, Boston, MA, USA.
medRxiv. 2020 Aug 25:2020.08.23.20178236. doi: 10.1101/2020.08.23.20178236.
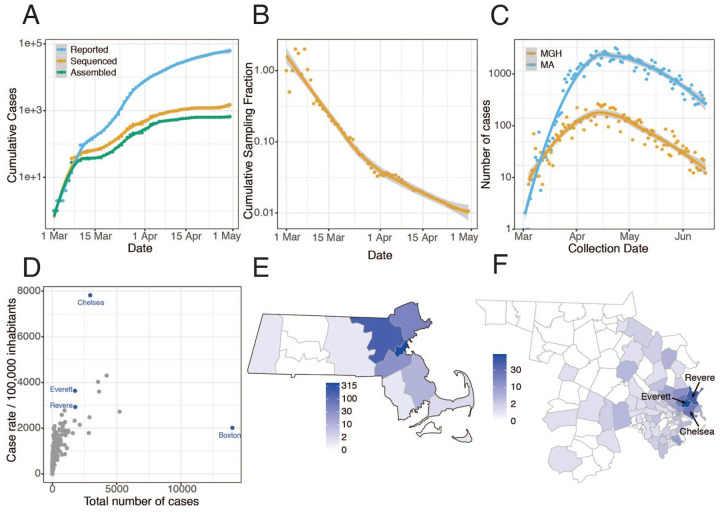
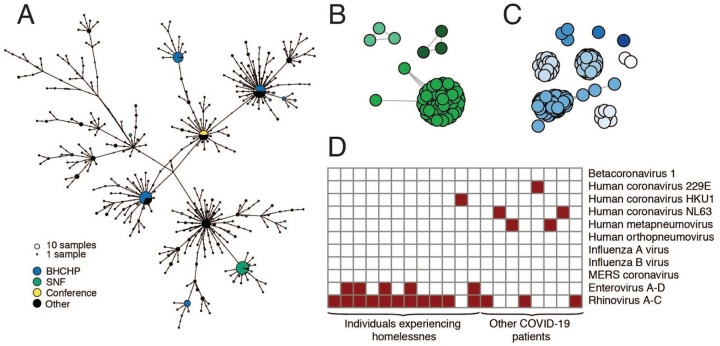
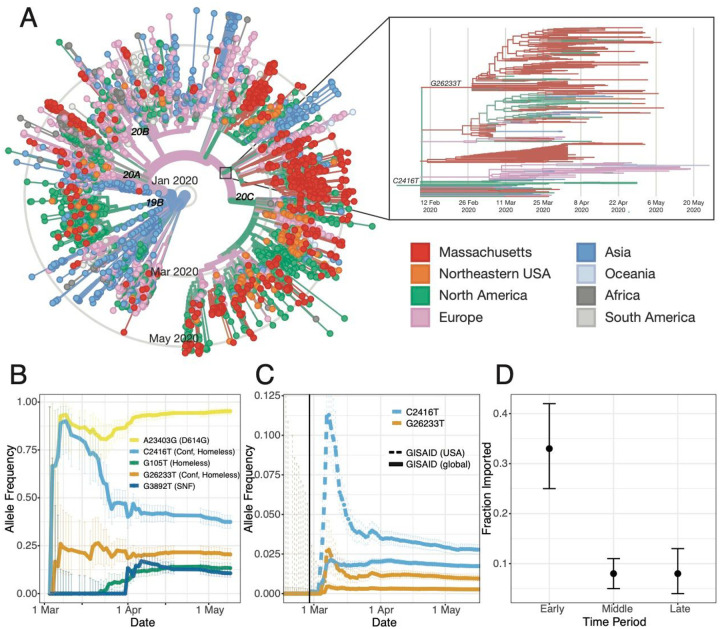
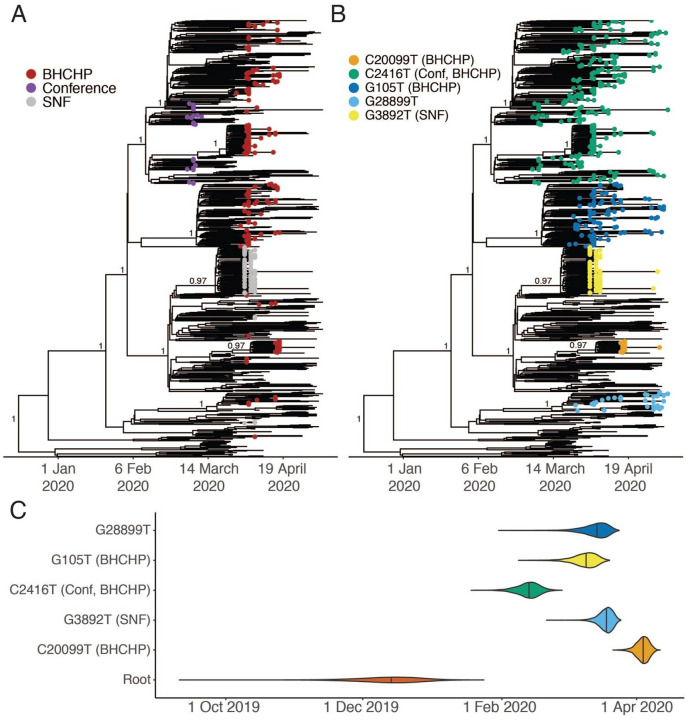
SARS-CoV-2 has caused a severe, ongoing outbreak of COVID-19 in Massachusetts with 111,070 confirmed cases and 8,433 deaths as of August 1, 2020. To investigate the introduction, spread, and epidemiology of COVID-19 in the Boston area, we sequenced and analyzed 772 complete SARS-CoV-2 genomes from the region, including nearly all confirmed cases within the first week of the epidemic and hundreds of cases from major outbreaks at a conference, a nursing facility, and among homeless shelter guests and staff. The data reveal over 80 introductions into the Boston area, predominantly from elsewhere in the United States and Europe. We studied two superspreading events covered by the data, events that led to very different outcomes because of the timing and populations involved. One produced rapid spread in a vulnerable population but little onward transmission, while the other was a major contributor to sustained community transmission, including outbreaks in homeless populations, and was exported to several other domestic and international sites. The same two events differed significantly in the number of new mutations seen, raising the possibility that SARS-CoV-2 superspreading might encompass disparate transmission dynamics. Our results highlight the failure of measures to prevent importation into MA early in the outbreak, underscore the role of superspreading in amplifying an outbreak in a major urban area, and lay a foundation for contact tracing informed by genetic data.
截至2020年8月1日,严重急性呼吸综合征冠状病毒2(SARS-CoV-2)在马萨诸塞州引发了持续的新冠肺炎疫情大爆发,确诊病例达111,070例,死亡8,433例。为调查新冠肺炎在波士顿地区的传入、传播及流行病学特征,我们对该地区772个完整的SARS-CoV-2基因组进行了测序和分析,其中包括疫情第一周内几乎所有的确诊病例,以及会议、护理机构、无家可归者收容所的客人和工作人员中数百例重大疫情爆发的病例。数据显示,有超过80起传入事件进入波士顿地区,主要来自美国其他地区和欧洲。我们研究了数据涵盖的两起超级传播事件,由于涉及的时间和人群不同,这两起事件导致了截然不同的结果。一起事件在脆弱人群中迅速传播,但后续传播很少,而另一起事件则是社区持续传播的主要原因,包括在无家可归者群体中的疫情爆发,并传播到了其他几个国内和国际地点。这两起事件在新出现的突变数量上有显著差异,这增加了SARS-CoV-2超级传播可能包含不同传播动态的可能性。我们的结果凸显了疫情爆发初期预防病毒传入马萨诸塞州的措施的失败,强调了超级传播在大城市地区扩大疫情中的作用,并为基于基因数据的接触者追踪奠定了基础。