Yu Dongwoo, Choi Joon Hyuk, Jeon Ikchan
Department of Neurosurgery.
Department of Pathology, Yeungnam University Hospital, Yeungnam University College of Medicine, Daegu, South Korea.
Medicine (Baltimore). 2020 Aug 14;99(33):e21741. doi: 10.1097/MD.0000000000021741.
Hemangiomas are usually found in cutaneous or mucosal layers, less than 1% of hemangiomas develop in skeletal muscles. Intramuscular hemangioma (IH) in the head and neck areas is relatively infrequent, accounting for 15% of IH. Most of them are identified as a benign mass, and rapid changes in size or internal bleeding are rare.
A 60-year-old female patient presented with a 2-week history of sudden onset posterior neck pain. There was no neurological deficit except limited neck motion due to pain. The palpable mass was noted on the paraspinal muscles of cervicothoracic junction, which was located midline to left side portion with tenderness.
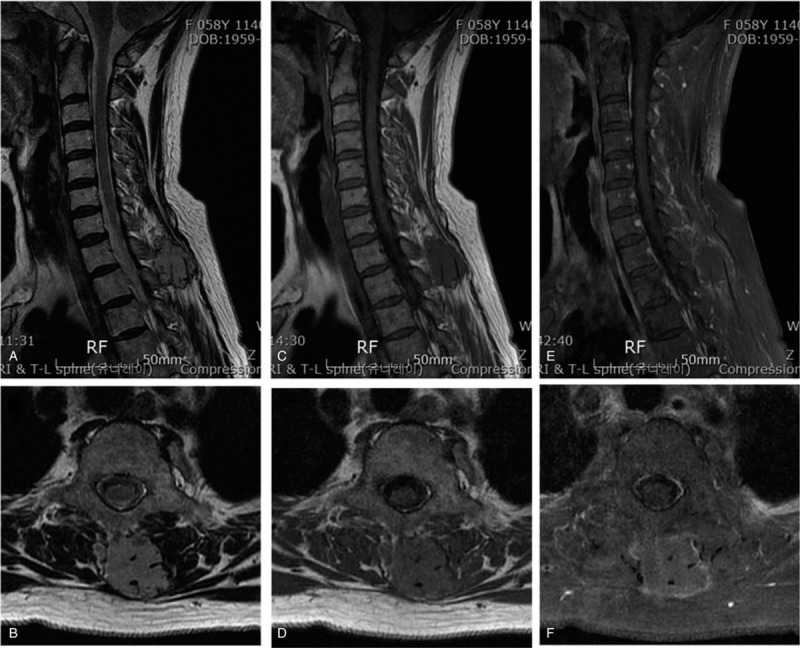
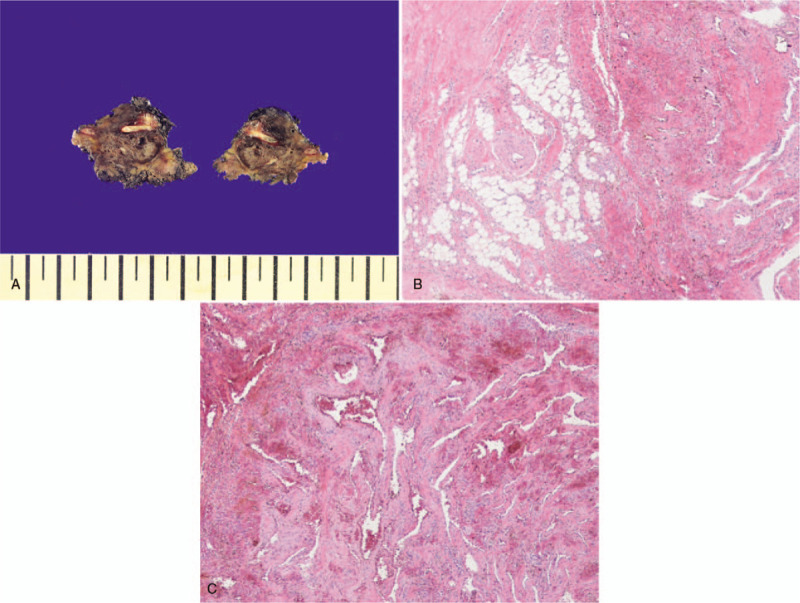
Magnetic resonance imaging demonstrated a round shaped, multi-lobulated, and well-defined mass lesion (4.1 × 2.6 × 0.9 cm) embedded from the inter-spinous space of T1-2 to the left paraspinal muscles. The lesion was iso-intense on T2-weighted images (WI), iso- to slightly low-intense on T1-WI, heterogeneous enhancement of intra- and peri-mass lesion on contrast-enhanced T1-WI. Vascular structures presented as signal voids were identified internally and around the mass lesion. Histological examination revealed a mixed-type hemangioma.
The mass was removed completely including some of the surrounding muscles where boundaries were unclear between the mass and surrounding muscles with ligation of peritumoral vessels. Dark-brown colored blood was drained from the ruptured tumor capsule during the dissection. There was no bony invasion.
The preoperative symptoms improved immediately after the operation. There is no residual or recurrence lesion by the 15-months follow-up.
IH with hemorrhagic transformation in the head and neck is extremely rare. In the case of intramuscular tumors accompanied by a sudden onset of severe acute pain, we recommend considering a differential diagnosis of IH with hemorrhagic transformation. Complete resection of the tumor mass including surrounding muscles is required to prevent recurrence.
血管瘤通常位于皮肤或黏膜层,不到1%的血管瘤发生于骨骼肌。头颈部肌内血管瘤(IH)相对少见,占肌内血管瘤的15%。大多数被认为是良性肿块,其大小快速变化或内部出血很少见。
一名60岁女性患者,有2周突发后颈部疼痛病史。除因疼痛导致颈部活动受限外,无神经功能缺损。在颈胸交界处的椎旁肌可触及肿块,位于中线左侧部分,有压痛。
磁共振成像显示一个圆形、多叶状、边界清晰的肿块病变(4.1×2.6×0.9cm),从T1-2棘突间隙延伸至左侧椎旁肌。该病变在T2加权图像(WI)上呈等信号,在T1-WI上呈等信号至略低信号,在增强T1-WI上肿块内部及周围病变呈不均匀强化。在肿块病变内部和周围可识别出呈信号缺失的血管结构。组织学检查显示为混合型血管瘤。
完整切除肿块,包括一些肿块与周围肌肉边界不清的周围肌肉,并结扎肿瘤周围血管。在解剖过程中,从破裂的肿瘤包膜中引出深褐色血液。无骨质侵犯。
术后术前症状立即改善。随访15个月无残留或复发病变。
头颈部伴有出血性转化的肌内血管瘤极为罕见。对于伴有突然发作的严重急性疼痛的肌内肿瘤,建议考虑鉴别诊断为伴有出血性转化的肌内血管瘤。需要完整切除肿瘤肿块及周围肌肉以防止复发。