Division of Nephrology, Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Republic of Korea.
PLoS One. 2020 Sep 3;15(9):e0238177. doi: 10.1371/journal.pone.0238177. eCollection 2020.
Renal hyperfiltration (RHF) has been found to be an independent predictor of adverse cardiovascular outcome. However, it remains uncertain whether it is precursor of chronic kidney disease (CKD) in a healthy population.
To determine relative risks and identify the predictor of incident proteinuria and decline of estimated glomerular filtration rate (eGFR) in subjects with RHF. A total of 55,992 subjects aged ≥20 years who underwent health check-up during 2004-2017 were included. Among them, 16,946 subjects who completed at least two health checkups were analyzed.
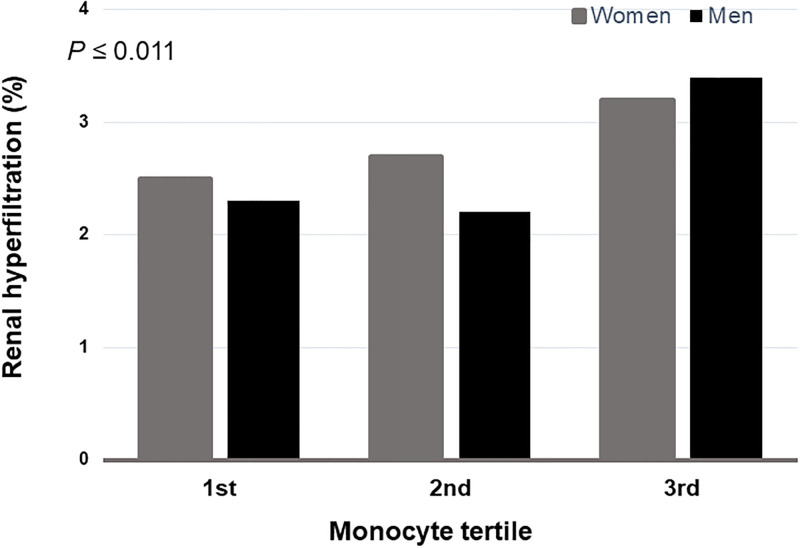
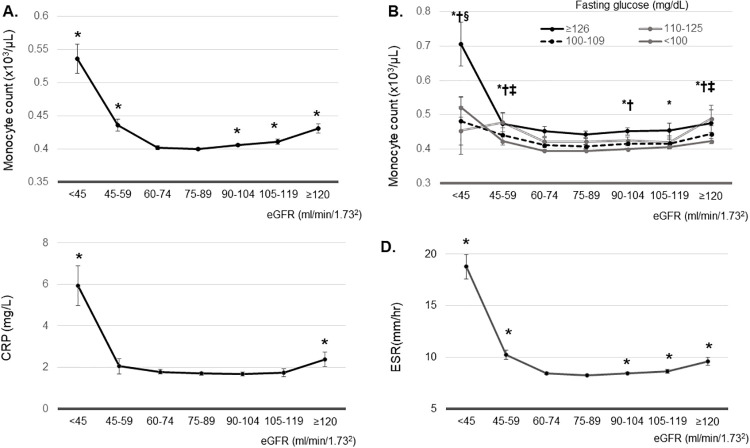
A total of 949 (5.6%) subjects developed proteinuria and 98 (0.6%) subjects showed ≥ 30% of eGFR decline. The risk of incident proteinuria was significantly higher in those with RHF (RR: 1.644; 95% CI: 1.064-2.541). Those with RHF showed 8.720 fold (95% CI: 4.205-18.081) increased risk for ≥30% decline. ESR, CRP, and monocyte count showed reversed J shaped curve according to the increase of eGFR. The adjusted mean of monocyte count was significantly higher in participants with eGFR ≥90ml/min/1.73m2 or < 60ml/min/1.73m2 compared to that in patients with eGFR 75-89ml/min/1.73m2. Compared to subjects with the lowest tertile of monocyte and no RHF, those with the highest tertile of monocyte count in the RHF group had 3.314-fold (95% CI: 1.893-5.802) higher risk of incident proteinuria and 3.822-fold (95% CI, 1.327-11.006) risk of 30% eGFR decline.
RHF had significantly increased risk of developing proteinuria and CKD in healthy subjects. Higher monocyte count might be used as a predictor of CKD in subjects with RHF.
肾高滤过(RHF)已被发现是不良心血管结局的独立预测因子。然而,在健康人群中,它是否是慢性肾脏病(CKD)的前兆尚不确定。
确定 RHF 患者发生蛋白尿和估算肾小球滤过率(eGFR)下降的相对风险,并识别其预测因素。共纳入 2004 年至 2017 年期间接受健康检查的年龄≥20 岁的 55992 例受试者。其中,分析了至少完成两次健康检查的 16946 例受试者。
共有 949 例(5.6%)受试者发生蛋白尿,98 例(0.6%)受试者 eGFR 下降≥30%。RHF 患者发生蛋白尿的风险明显更高(RR:1.644;95%CI:1.064-2.541)。RHF 患者 eGFR 下降≥30%的风险增加 8.720 倍(95%CI:4.205-18.081)。根据 eGFR 的增加,ESR、CRP 和单核细胞计数显示出相反的 J 形曲线。与 eGFR 为 75-89ml/min/1.73m2 或<60ml/min/1.73m2 的患者相比,eGFR≥90ml/min/1.73m2 或<60ml/min/1.73m2 的患者的单核细胞计数的调整均值明显更高。与单核细胞最低三分位和无 RHF 的受试者相比,RHF 组中单核细胞计数最高三分位的受试者发生蛋白尿的风险增加 3.314 倍(95%CI:1.893-5.802),eGFR 下降 30%的风险增加 3.822 倍(95%CI,1.327-11.006)。
RHF 显著增加了健康受试者发生蛋白尿和 CKD 的风险。较高的单核细胞计数可能可作为 RHF 患者 CKD 的预测指标。