Rokaya Dinesh, Srimaneepong Viritpon, Wisitrasameewon Wichaya, Humagain Manoj, Thunyakitpisal Pasutha
International College of Dentistry, Walailak University, Bangkok, Thailand.
Research Unit of Herbal Medicine, Biomaterials and Materials for Dental Treatment, Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand.
Eur J Dent. 2020 Oct;14(4):672-682. doi: 10.1055/s-0040-1715779. Epub 2020 Sep 3.
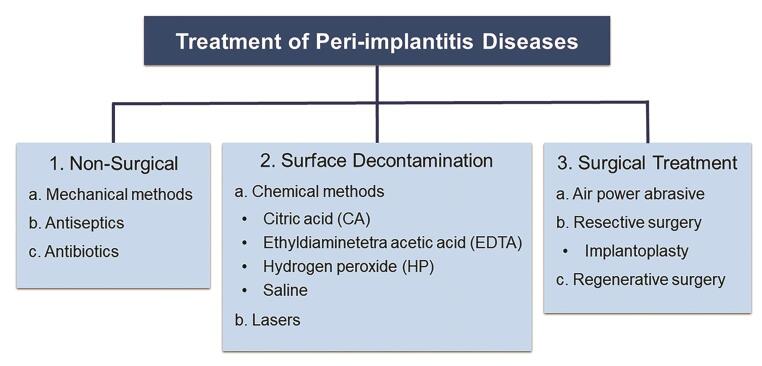
Despite the success rates of dental implants, peri-implantitis presents as the most common complication in implant dentistry. This review discusses various factors associated with peri-implantitis and various available treatments, highlighting their advantages and disadvantages. Relevant articles on peri-implantitis published in English were reviewed from August 2010 to April 2020 in MEDLINE/PubMed, Scopus, and ScienceDirect. The identified risk indicators of peri-implant diseases are plaque, smoking, history of periodontitis, surface roughness, residual cement, emergence angle >30 degrees, radiation therapy, keratinized tissue width, and function time of the implant, sex, and diabetes. Peri-implantitis treatments can be divided into nonsurgical (mechanical, antiseptic, and antibiotics), surface decontamination (chemical and laser), and surgical (air powder abrasive, resective, and regenerative). However, mechanical debridement alone may fail to eliminate the causative bacteria, and this treatment should be combined with other treatments (antiseptics and surgical treatment). Surface decontamination using chemical agents may be used as an adjuvant treatment; however, the definitive clinical benefit is yet not proven. Laser treatment may result in a short-term decrease in periodontal pocket depth, while air powder abrasive is effective in cleaning a previously contaminated implant surface. Surgical elimination of a pocket, bone recontouring and plaque control are also effective for treating peri-implantitis. The current evidence indicates that regenerative approaches to treat peri-implant defects are unpredictable.
尽管牙种植体成功率较高,但种植体周围炎仍是种植牙科中最常见的并发症。本文综述了与种植体周围炎相关的各种因素及现有的各种治疗方法,重点阐述了它们的优缺点。2010年8月至2020年4月期间,在MEDLINE/PubMed、Scopus和ScienceDirect数据库中检索了以英文发表的关于种植体周围炎的相关文章。已确定的种植体周围疾病风险指标包括菌斑、吸烟、牙周炎病史、表面粗糙度、残留粘固剂、穿出角度>30度、放射治疗、角化组织宽度、种植体功能时间、性别和糖尿病。种植体周围炎的治疗方法可分为非手术治疗(机械、抗菌和抗生素治疗)、表面去污(化学和激光)和手术治疗(气粉磨蚀、切除和再生)。然而,单纯的机械清创可能无法消除致病细菌,这种治疗应与其他治疗方法(抗菌和手术治疗)相结合。使用化学剂进行表面去污可作为辅助治疗;然而,其确切的临床益处尚未得到证实。激光治疗可能会使牙周袋深度短期内降低,而气粉磨蚀对清洁先前受污染的种植体表面有效。手术消除牙周袋、骨轮廓修整和菌斑控制对治疗种植体周围炎也有效。目前的证据表明,治疗种植体周围缺损的再生方法效果难以预测。