National Cancer Institute/Pediatric Oncology Branch, National Institutes of Health, Bethesda, Maryland, USA
National Heart, Lung, and Blood Institute/Cardiovascular Branch, National Institutes of Health, Bethesda, Maryland, USA.
J Immunother Cancer. 2020 Sep;8(2). doi: 10.1136/jitc-2020-001159.
Chimeric antigen receptor (CAR) T-cell-associated cytokine release syndrome (CRS) may present with tachycardia, hemodynamic instability and reduced cardiac function. Pediatric CAR studies examining cardiac toxicity are limited.
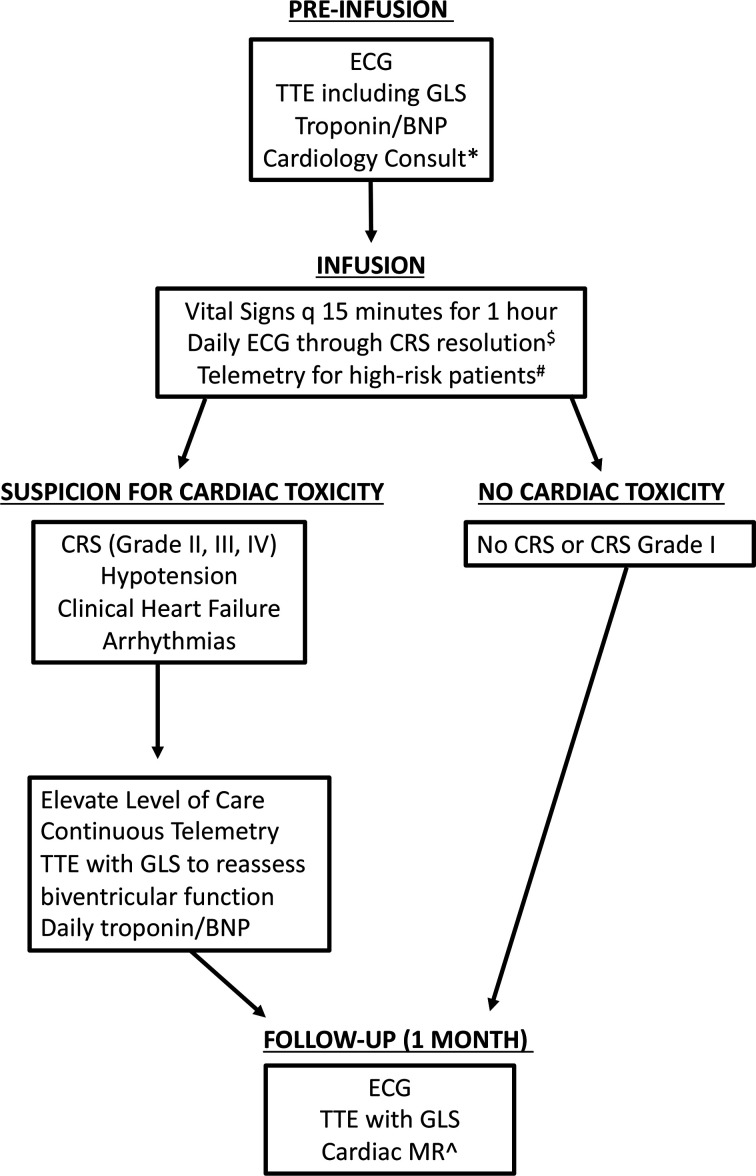
We report on cardiac toxicity observed in children and young adults with hematologic malignancies enrolled in a CD19-28ζ CAR T-cell phase I trial (NCT01593696). All patients had a formal baseline echocardiogram. Real-time studies included echocardiograms on intensive care unit (ICU) transfer, and serial troponin and pro-B-type natriuretic peptide (pro-BNP) in the select patients.
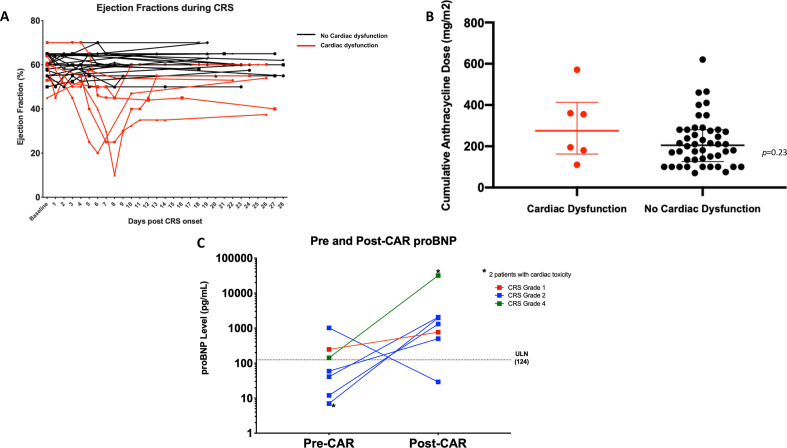
From July 2012 to March 2016, 52 patients, with a median age of 13.4 years (range 4.2-30.3) were treated. CRS developed in 37/52 (71%), which was grade 3-4 CRS in nine patients (17%). The median prior anthracycline exposure was 205 mg/m (range 70-620 mg/m) in doxorubicin equivalents. The median baseline left ventricle ejection fraction (LVEF) and baseline LV global longitudinal strain (GLS) were 60% (range 50%-70%) and 16.8% (range 14.1%-23.5%, n=37) respectively. The majority, 78% (29/37), of patients had a reduced GLS <19% at baseline, and 6% (3/52) of patients had baseline LVEF <53%. ICU transfers occurred in 21 patients, with nine requiring vasoactive hemodynamic support and three necessitating >1 vasopressor. Six (12%) patients developed cardiac dysfunction (defined by >10% absolute decrease in LVEF or new-onset grade 2 or higher LV dysfunction, per CTCAE v4), among whom 4 had grade 3-4 CRS. Troponin elevations were seen in 4 of 13 patients, all of whom had low LVEF. Pro-BNP was elevated from baseline in 6/7 patients at the onset of CRS, with higher levels correlating with more severe CRS. Cardiac dysfunction fully resolved in all but two patients by day 28 post-CAR.
Cardiac toxicity related to CD19-28ζ CAR T-cell-associated CRS was generally reversible by day 28 postinfusion. Implementation of more frequent monitoring with formal echocardiograms incorporating systemic analysis of changes in GLS, and cardiac biomarkers (troponin and proBNP) may help to earlier identify those patients at highest risk of severe cardiac systolic dysfunction, facilitating earlier interventions for CRS to potentially mitigate acute cardiac toxicity.
嵌合抗原受体(CAR)T 细胞相关细胞因子释放综合征(CRS)可能表现为心动过速、血流动力学不稳定和心功能降低。儿科 CAR 研究中对心脏毒性的研究有限。
我们报告了在接受 CD19-28ζ CAR T 细胞 I 期试验(NCT01593696)的血液系统恶性肿瘤儿童和青少年中观察到的心脏毒性。所有患者均进行了正式的基线超声心动图检查。实时研究包括 ICU 转移时的超声心动图检查,以及在选择的患者中连续检测肌钙蛋白和 pro-B 型利钠肽(pro-BNP)。
从 2012 年 7 月至 2016 年 3 月,共治疗了 52 例中位年龄为 13.4 岁(范围 4.2-30.3)的患者。37/52 例(71%)发生 CRS,9 例(17%)为 3-4 级 CRS。中位既往蒽环类药物暴露量为多柔比星等效物 205mg/m(范围 70-620mg/m)。中位基线左心室射血分数(LVEF)和基线左心室整体纵向应变(GLS)分别为 60%(范围 50%-70%)和 16.8%(范围 14.1%-23.5%,n=37)。大多数患者(78%,29/37)基线 GLS<19%,6%(3/52)的患者基线 LVEF<53%。21 例患者发生 ICU 转移,其中 9 例需要血管活性血流动力学支持,3 例需要>1 种升压药。6 例(12%)患者出现心脏功能障碍(定义为 LVEF 绝对值下降>10%或新发 2 级或更高级别的 LV 功能障碍,按 CTCAE v4),其中 4 例为 3-4 级 CRS。13 例患者中有 4 例肌钙蛋白升高,所有患者的 LVEF 均较低。CRS 发病时,6/7 例患者的 pro-BNP 从基线升高,水平较高与 CRS 更严重相关。除 2 例患者外,所有患者的心脏功能障碍在 CAR 输注后 28 天内完全缓解。
与 CD19-28ζ CAR T 细胞相关 CRS 相关的心脏毒性在 CAR 输注后 28 天内通常是可逆的。通过更频繁的监测,包括正式的超声心动图检查,并对 GLS 的系统分析,以及心脏生物标志物(肌钙蛋白和 proBNP)的变化,可以帮助更早地识别那些发生严重心脏收缩功能障碍风险最高的患者,从而更早地进行 CRS 干预,可能减轻急性心脏毒性。