CEPED, Institute for Research on Sustainable Development, IRD-Université de Paris, ERL INSERM SAGESUD, Paris, France.
UNDP/UNFPA/UNICEF/World Bank Special Program of Research, Development and Research Training in Human Reproduction (HRP), Department of Sexual and Reproductive Health and Research, World Health Organization, Geneva, Switzerland.
Implement Sci. 2020 Sep 4;15(1):72. doi: 10.1186/s13012-020-01029-4.
While cesarean sections (CSs) are a life-saving intervention, an increasing number are performed without medical reasons in low- and middle-income countries (LMICs). Unnecessary CS diverts scarce resources and thereby reduces access to healthcare for women in need. Argentina, Burkina Faso, Thailand, and Vietnam are committed to reducing unnecessary CS, but many individual and organizational factors in healthcare facilities obstruct this aim. Nonclinical interventions can overcome these barriers by helping providers improve their practices and supporting women's decision-making regarding childbirth. Existing evidence has shown only a modest effect of single interventions on reducing CS rates, arguably because of the failure to design multifaceted interventions effectively tailored to the context. The aim of this study is to design, adapt, and test a multifaceted intervention for the appropriate use of CS in Argentina, Burkina Faso, Thailand, and Vietnam.
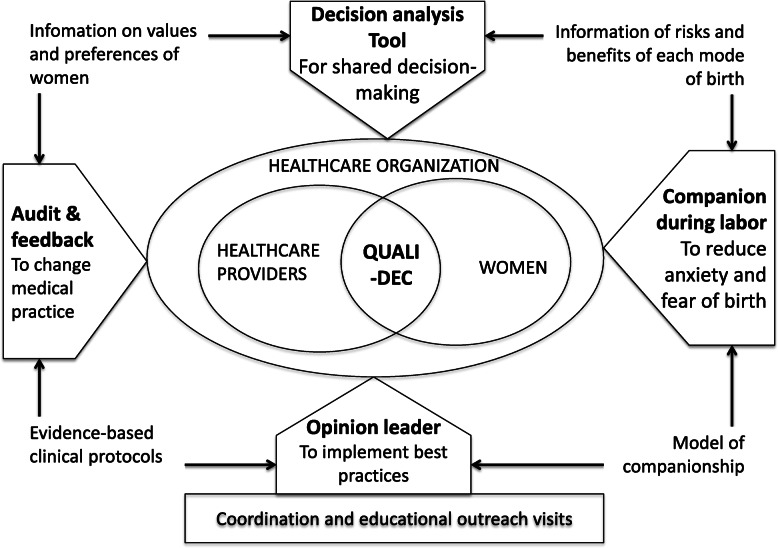
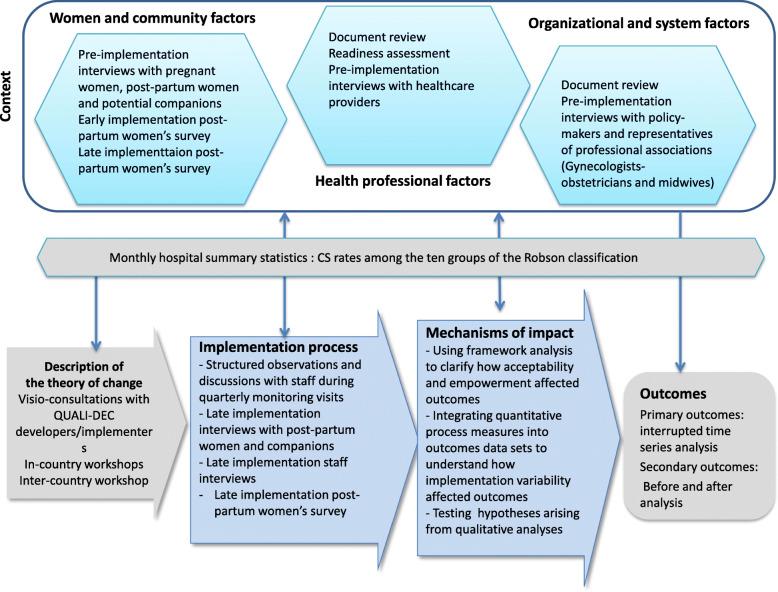
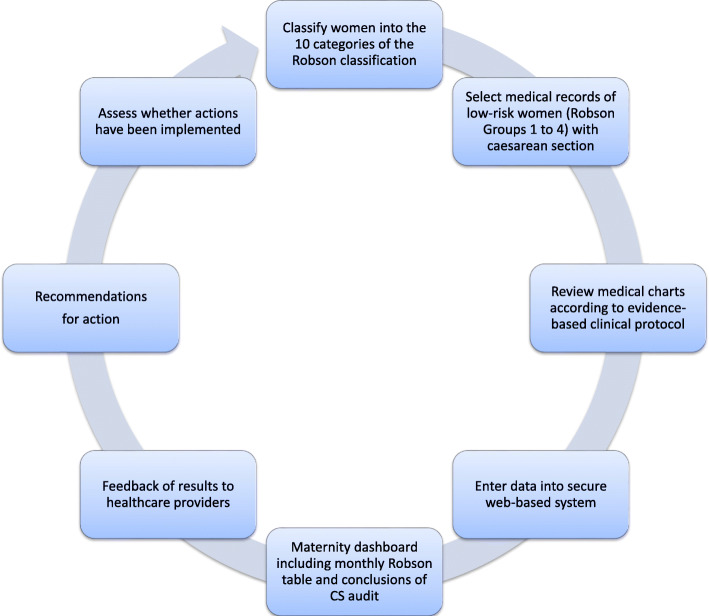
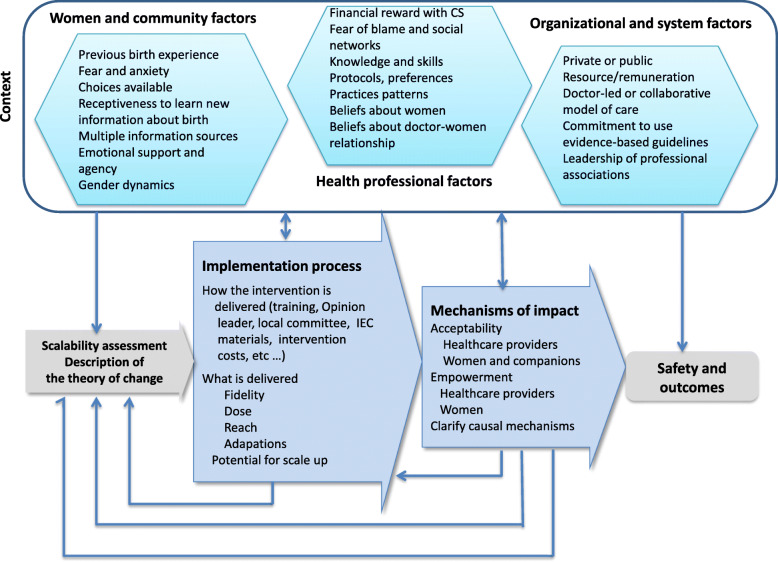
We designed an intervention (QUALIty DECision-making-QUALI-DEC) with four components: (1) opinion leaders at heathcare facilities to improve adherence to best practices among clinicians, (2) CS audits and feedback to help providers identify potentially avoidable CS, (3) a decision analysis tool to help women make an informed decision on the mode of birth, and (4) companionship to support women during labor. QUALI-DEC will be implemented and evaluated in 32 hospitals (8 sites per country) using a pragmatic hybrid effectiveness-implementation design to test our implementation strategy, and information regarding its impact on relevant maternal and perinatal outcomes will be gathered. The implementation strategy will involve the participation of women, healthcare professionals, and organizations and account for the local environment, needs, resources, and social factors in each country.
There is urgent need for interventions and implementation strategies to optimize the use of CS while improving health outcomes and satisfaction in LMICs. This can only be achieved by engaging all stakeholders involved in the decision-making process surrounding birth and addressing their needs and concerns. The study will generate robust evidence about the effectiveness and the impact of this multifaceted intervention. It will also assess the acceptability and scalability of the intervention and the capacity for empowerment among women and providers alike.
ISRCTN67214403.
剖宫产(CS)是一种救生干预措施,但在中低收入国家(LMIC),越来越多的 CS 是在没有医学原因的情况下进行的。不必要的 CS 会转移稀缺资源,从而减少有需要的妇女获得医疗保健的机会。阿根廷、布基纳法索、泰国和越南都致力于减少不必要的 CS,但医疗机构中的许多个人和组织因素阻碍了这一目标的实现。非临床干预可以通过帮助提供者改善实践并支持妇女在分娩方面做出决策来克服这些障碍。现有证据表明,单一干预措施对降低 CS 率的影响仅适度,这可能是因为未能有效地设计针对具体情况的多方面干预措施。本研究旨在为阿根廷、布基纳法索、泰国和越南设计、改编和测试一种多方面的干预措施,以合理使用 CS。
我们设计了一个干预措施(QUALIty DECision-making-QUALI-DEC),包括四个组成部分:(1)医疗机构的意见领袖,以提高临床医生遵守最佳实践的能力,(2)CS 审核和反馈,以帮助提供者识别潜在可避免的 CS,(3)决策分析工具,以帮助妇女就分娩方式做出明智的决定,(4)陪伴,以支持妇女分娩。QUALI-DEC 将在 32 家医院(每个国家 8 个地点)中实施和评估,采用实用混合有效性实施设计来测试我们的实施策略,并收集有关其对相关产妇和围产期结局的影响的信息。实施策略将涉及妇女、医疗保健专业人员和组织的参与,并考虑到每个国家的当地环境、需求、资源和社会因素。
迫切需要干预措施和实施策略来优化 CS 的使用,同时改善 LMIC 的健康结果和满意度。这只能通过让所有参与分娩决策过程的利益相关者参与进来,并满足他们的需求和关切来实现。该研究将产生关于这种多方面干预措施的有效性和影响的有力证据。它还将评估干预措施的可接受性和可扩展性,以及妇女和提供者赋权的能力。
ISRCTN67214403。