Department of Hematology, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, People's Republic of China.
Department of Hematology, Beijing Jishuitan Hospital, Beijing, China.
Ann Hematol. 2020 Nov;99(11):2589-2598. doi: 10.1007/s00277-020-04234-9. Epub 2020 Sep 6.
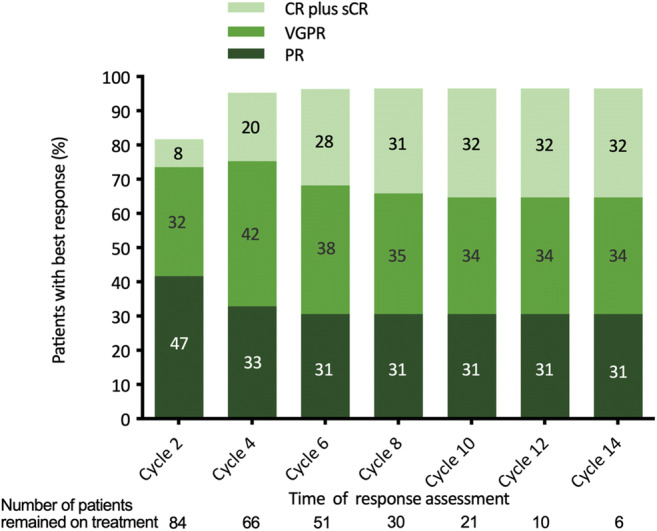
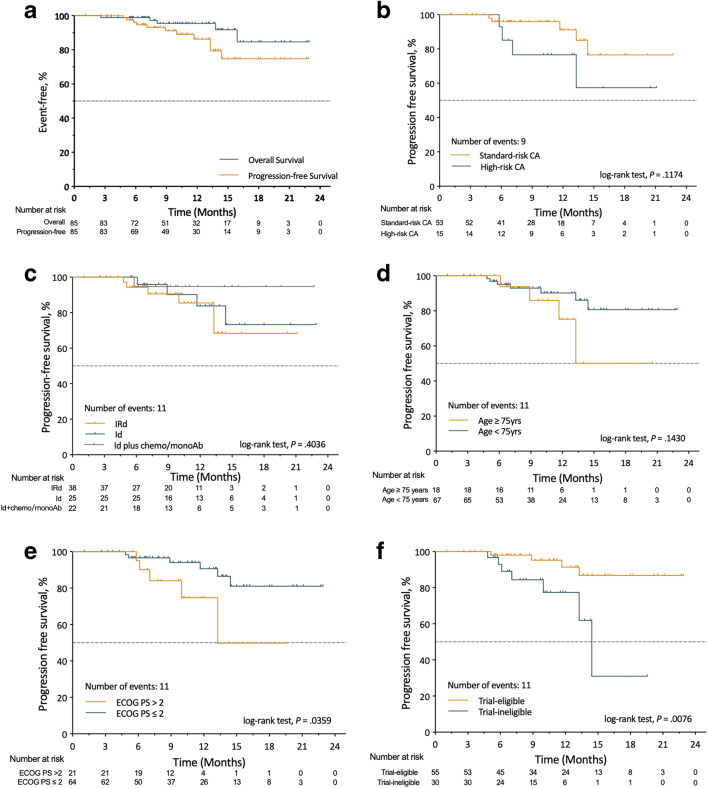
The induction therapy containing ixazomib, an oral proteasome inhibitor, has shown favorable efficacy and safety in clinical trials, but its experience in real-life remains limited. In routine practice, few patients received ixazomib-based induction therapy due to reasons including (1) patients' preference on oral regimens, (2) concerns on adverse events (AEs) of other intravenous/subcutaneous regimens, (3) requirements for less center visits, and (4) fears of COVID-19 and other infectious disease exposures. With the aim of assessing the real-life effectiveness and safety of ixazomib-based induction therapy, we performed this multi-center, observational study on 85 newly diagnosed multiple myeloma (NDMM) patients from 14 medical centers. Ixazomib-based regimens included ixazomib-lenalidomide-dexamethasone (IRd) in 44.7% of patients, ixazomib-dexamethasone (Id) in 29.4%, and Id plus another agent (doxorubicin, cyclophosphamide, thalidomide, or daratumumab) in 25.9%. Different ixazomib-based therapies were applied due to (1) financial burdens or limitations on local health insurance coverage, (2) concerns on treatment tolerance, and (3) drug accessibility issue. Ten patients received ixazomib maintenance. The median age was 67 years; 43.5% had ISS stage III disease; 48.2% had an Eastern Cooperative Oncology Group performance score ≥ 2; and 17.6% with high-risk cytogenetic abnormalities. Overall response rate for all 85 patients was 95.3%, including 65.9% very good partial response or better and 29.5% complete responses. The median time to response was 30 days. The response rate was similar across different ixazomib-based regimens. Median progression-free survival was not reached. Severe AEs (≥ grade 3) were reported in 29.4% of patients. No grade 3/4 peripheral neuropathy (PN) occurred. Patients received a median of 6 (range 1-20) cycles of ixazomib treatment; 56.6% remained on treatment at data cutoff; 15.3% discontinued treatment due to intolerable AEs. These results support that the ixazomib-based frontline therapy was highly effective with acceptable toxicity in routine practice and the ixazomib oral regimens could be good alternative options for NDMM patients.
含伊沙佐米的诱导治疗方案,一种口服蛋白酶体抑制剂,在临床试验中显示出良好的疗效和安全性,但其实践经验仍然有限。在常规实践中,由于以下原因,很少有患者接受伊沙佐米为基础的诱导治疗:(1)患者对口服方案的偏好,(2)对其他静脉/皮下方案不良事件(AE)的担忧,(3)对减少中心就诊次数的要求,以及(4)对 COVID-19 和其他传染病暴露的恐惧。为了评估基于伊沙佐米的诱导治疗的真实有效性和安全性,我们对来自 14 家医疗中心的 85 例新诊断多发性骨髓瘤(NDMM)患者进行了这项多中心、观察性研究。基于伊沙佐米的方案包括 44.7%的患者使用伊沙佐米-来那度胺-地塞米松(IRd)、29.4%的患者使用伊沙佐米-地塞米松(Id),以及 25.9%的患者使用 Id 加另一种药物(多柔比星、环磷酰胺、沙利度胺或达雷妥尤单抗)。不同的伊沙佐米治疗方案是基于以下原因应用的:(1)经济负担或当地医疗保险覆盖范围的限制,(2)对治疗耐受性的关注,以及(3)药物可及性问题。10 例患者接受了伊沙佐米维持治疗。中位年龄为 67 岁;43.5%的患者为 ISS Ⅲ期疾病;48.2%的患者东部合作肿瘤学组(ECOG)体能状态评分≥2;17.6%的患者存在高危细胞遗传学异常。85 例患者的总体缓解率为 95.3%,包括 65.9%的非常好部分缓解或更好和 29.5%的完全缓解。中位缓解时间为 30 天。不同的伊沙佐米方案的缓解率相似。中位无进展生存期未达到。报告了 29.4%的患者发生严重不良事件(≥3 级)。未发生 3/4 级周围神经病变(PN)。患者接受了中位数为 6 个(范围 1-20)周期的伊沙佐米治疗;56.6%的数据截止时仍在接受治疗;15.3%因无法耐受的不良事件而停止治疗。这些结果表明,伊沙佐米为基础的一线治疗在常规实践中具有高度有效性和可接受的毒性,伊沙佐米口服方案可为 NDMM 患者提供良好的替代选择。