Section for Comparative Pediatrics and Nutrition, University of Copenhagen, Copenhagen, Denmark.
Front Immunol. 2020 Aug 13;11:1808. doi: 10.3389/fimmu.2020.01808. eCollection 2020.
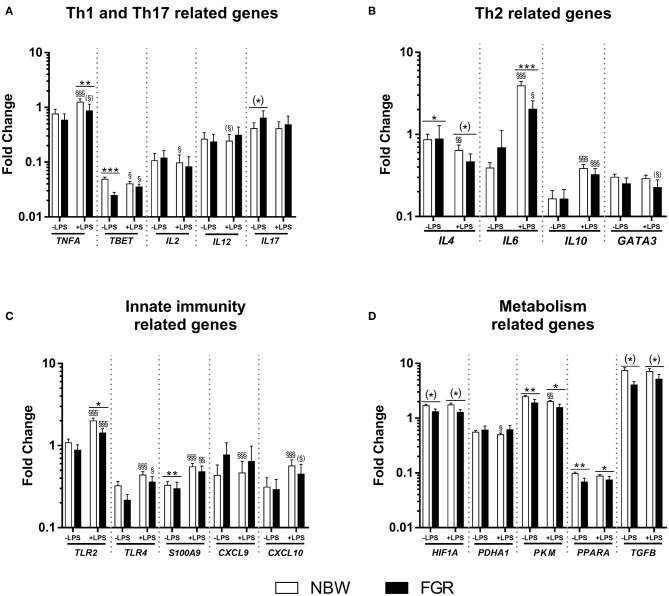
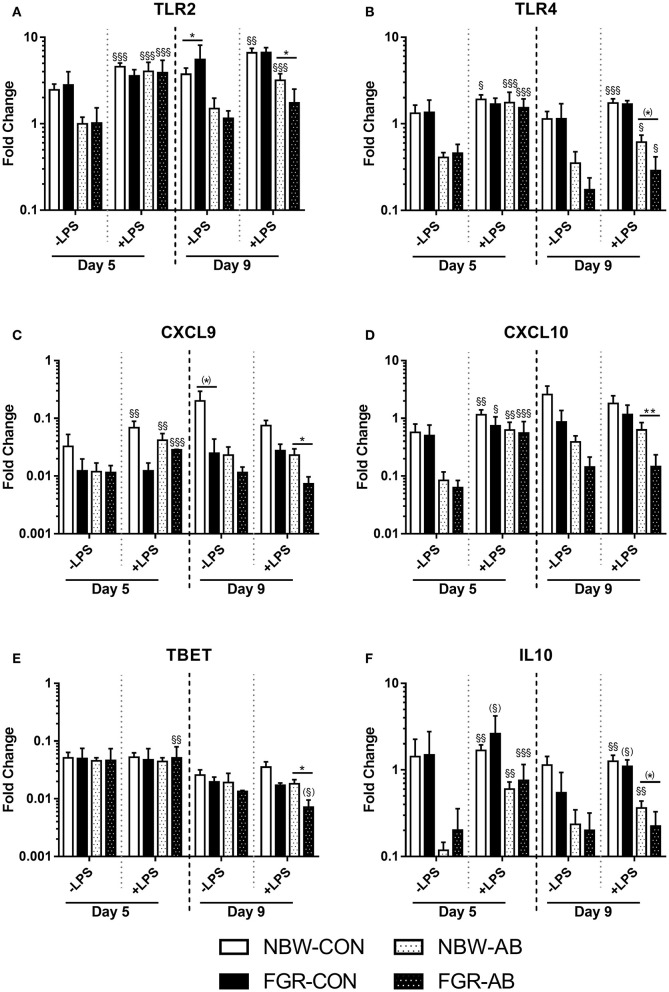
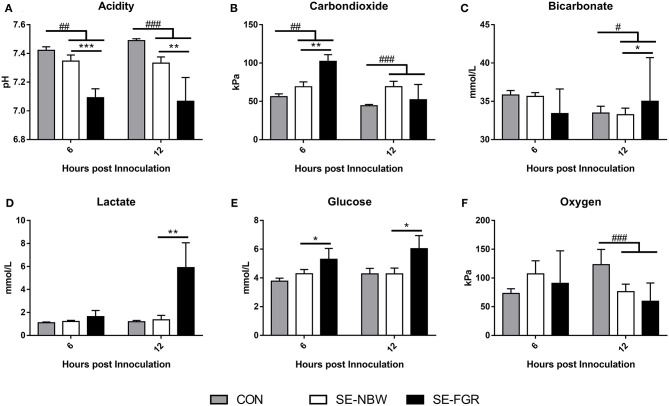
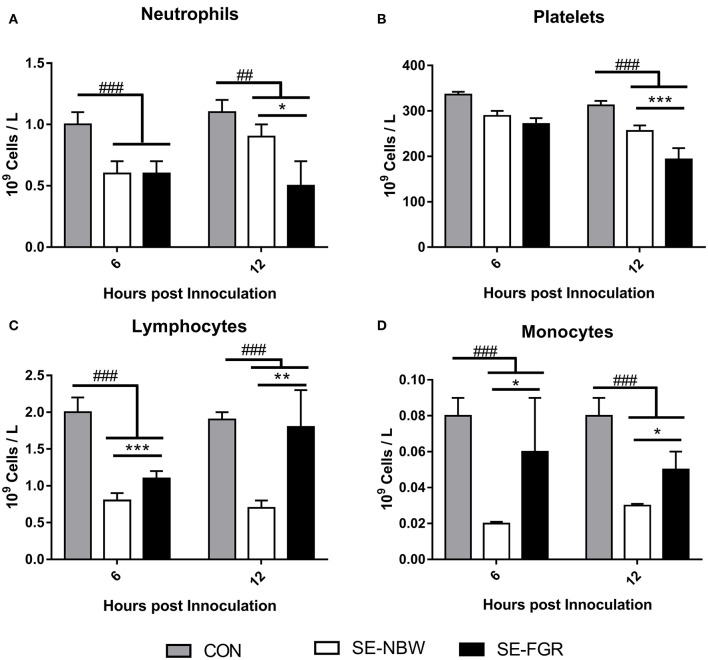
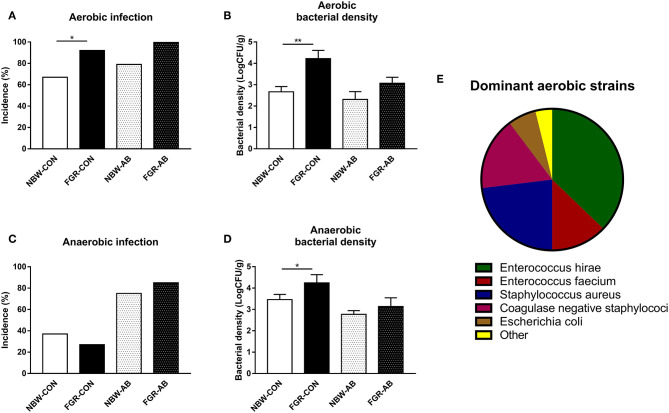
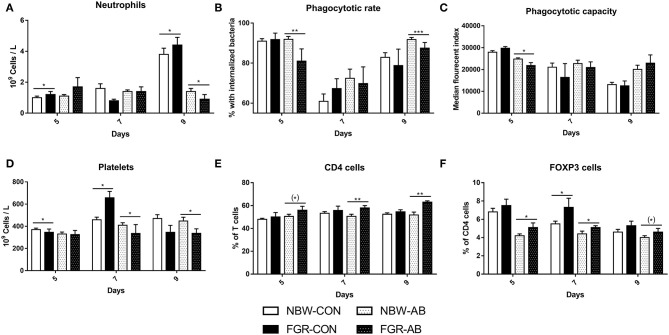
Infants born preterm or small for gestational age (SGA, due to fetal growth restriction) both show an increased risk of neonatal infection. However, it remains unclear how the co-occurrence of preterm birth and SGA may affect neonatal immunity and infection risk. We hypothesized that fetal growth restricted (FGR) preterm newborns possess impaired immune competence and increased susceptibility to systemic infection and sepsis, relative to corresponding normal birth weight (NBW) newborns. Using preterm pigs as a model for preterm infants, gene expression in lipopolysaccharide (LPS) stimulated cord blood was compared between NBW and FGR (lowest 25% birth weight percentile) preterm pigs. Next, clinical responses to a systemic (SE) challenge were investigated in newborn FGR and NBW preterm pigs. Finally, occurrence of spontaneous infections were investigated in 9 d-old FGR and NBW preterm pigs, with or without neonatal antibiotics treatment. At birth, preterm FGR piglets showed diminished cord blood responses to LPS for genes related to both innate and adaptive immunity, and also more severe septic responses following SE infection (e.g., higher blood lactate, decreased blood pH, neutrophil and platelet counts, relative to NBW pigs). After 9 d, FGR pigs had higher incidence and severity of spontaneous infections (e.g., higher bacterial densities in the bone marrow), increased regulatory T cell numbers, reduced neutrophil phagocytosis capacity, and impaired blood gene responses to LPS, especially when receiving neonatal antibiotics. FGR at preterm birth is associated with poor immune competence, impaired infection resistance, and greater sepsis susceptibility in the immediate postnatal period. Our results may explain the increased morbidity and mortality of SGA preterm infants and highlight the need for clinical vigilance for this highly sensitive subgroup of preterm neonates.
早产儿或因胎儿生长受限而出生体重小于胎龄儿(SGA)均有发生新生儿感染的风险增加。然而,目前尚不清楚早产和 SGA 的共同发生如何影响新生儿的免疫和感染风险。我们假设胎儿生长受限(FGR)的早产儿具有免疫功能受损和对全身感染和败血症的易感性增加,相对于相应的正常出生体重(NBW)的新生儿。 我们使用早产猪作为早产儿模型,比较了 NBW 和 FGR(出生体重最低 25%百分位)早产猪的脂多糖(LPS)刺激脐带血中的基因表达。接下来,我们研究了新生儿 FGR 和 NBW 早产猪对全身(SE)挑战的临床反应。最后,我们研究了 9 日龄 FGR 和 NBW 早产猪在有无新生儿抗生素治疗的情况下自发性感染的发生情况。 在出生时,FGR 早产仔猪的脐带血对 LPS 的反应减弱,与先天和适应性免疫相关的基因减少,并且在 SE 感染后出现更严重的败血症反应(例如,血乳酸升高,血 pH 值降低,中性粒细胞和血小板计数减少,与 NBW 仔猪相比)。9 天后,FGR 仔猪自发性感染的发生率和严重程度更高(例如,骨髓中的细菌密度更高),调节性 T 细胞数量增加,中性粒细胞吞噬能力降低,以及 LPS 诱导的血液基因反应受损,尤其是在接受新生儿抗生素治疗时。 早产时的 FGR 与出生后即刻的免疫功能受损、感染抵抗力降低和败血症易感性增加有关。我们的结果可以解释 SGA 早产儿发病率和死亡率增加的原因,并强调需要对这一高度敏感的早产儿亚组保持临床警惕。