Shah Vishank Arun, Nalleballe Krishna, Zaghlouleh Mhd Ezzat, Onteddu Sanjeeva
University of Arkansas for Medical Sciences, USA.
Brain Behav Immun Health. 2020 Oct;8:100136. doi: 10.1016/j.bbih.2020.100136. Epub 2020 Sep 1.
Acute encephalopathy with COVID-19 has been reported in several studies but its impact on outcomes remains unclear. We hypothesized that hospitalized COVID-19 patients with encephalopathy have worse COVID-19 related outcomes.
We used TriNetX, with a large COVID-19 database, collecting real-time electronic medical records data. We included hospitalized COVID-19 patients since January 20, 2020 who had encephalopathy based on ICD-10 coding. We examined clinical outcomes comprising need for critical care services, intubation and mortality among these patients and compared it with patients without encephalopathy before and after propensity-score matching.
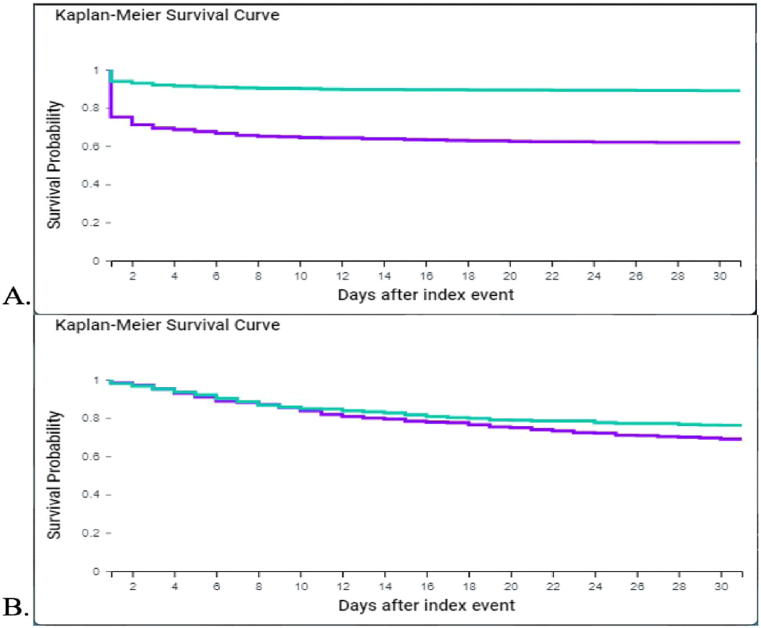
Of 12,601 hospitalized COVID-19 patients, 1092 (8.7%) developed acute encephalopathy. Patients in the acute encephalopathy group were older (67 vs. 61 years) and had higher prevalence of medical co-morbidities including obesity, hypertension, diabetes, heart disease, COPD, chronic kidney and liver disease among others. Before and after propensity score-matching for co-morbidities, patients with acute encephalopathy were more likely to need critical care services (35.6% vs. 16.9%, p < 0.0001), intubation (19.5% vs. 6.0%, p < 0.0001) and had higher 30-day mortality (24.3% vs. 17.9%, p 0.0002).
Among hospitalized COVID-19 patients, acute encephalopathy is common and more likely to occur in patients with medical co-morbidities and are more likely to need critical care, intubation and have higher 30-day mortality even after adjusting for age and underlying medical co-morbidities.
多项研究报告了新型冠状病毒肺炎(COVID-19)相关的急性脑病,但它对预后的影响仍不清楚。我们推测,患有脑病的COVID-19住院患者有更差的COVID-19相关预后。
我们使用了TriNetX,其拥有一个大型COVID-19数据库,收集实时电子病历数据。我们纳入了自2020年1月20日起因国际疾病分类第十版(ICD-10)编码诊断为脑病的COVID-19住院患者。我们检查了这些患者的临床结局,包括对重症监护服务的需求、插管情况和死亡率,并在倾向评分匹配前后将其与无脑病的患者进行比较。
在12,601例COVID-19住院患者中,1092例(8.7%)发生了急性脑病。急性脑病组患者年龄更大(67岁对61岁),合并症患病率更高,包括肥胖、高血压、糖尿病、心脏病、慢性阻塞性肺疾病(COPD)、慢性肾脏和肝脏疾病等。在对合并症进行倾向评分匹配前后,急性脑病患者更有可能需要重症监护服务(35.6%对16.9%,p<0.0001)、插管(19.5%对6.0%,p<0.0001),且30天死亡率更高(24.3%对17.9%,p = 0.0002)。
在COVID-19住院患者中,急性脑病很常见,更易发生于有合并症的患者,并且即使在调整年龄和潜在合并症后,仍更有可能需要重症监护、插管,且30天死亡率更高。