Departments of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City, Utah, Northwestern University, Chicago, Illinois, University of Alabama at Birmingham, Birmingham, Alabama, Stanford University, Stanford, California, Columbia University, New York, New York, Brown University, Providence, Rhode Island, University of Texas Medical Branch, Galveston, Texas, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, University of Texas Health Science Center at Houston-Children's Memorial Hermann Hospital, Houston, Texas, The Ohio State University, Columbus, Ohio, MetroHealth Medical Center-Case Western Reserve University, Cleveland, Ohio, University of Texas Southwestern Medical Center, Dallas, Texas, University of Colorado School of Medicine, Anschutz Medical Campus, Aurora, Colorado, University of Pennsylvania, Philadelphia, Pennsylvania, Duke University, Durham, North Carolina, University of Pittsburgh, Pittsburgh, Pennsylvania, and Washington University in St. Louis, St. Louis, Missouri; the George Washington University Biostatistics Center, Washington, DC; and the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Maryland.
Obstet Gynecol. 2020 Oct;136(4):698-705. doi: 10.1097/AOG.0000000000004046.
To develop models to predict vaginal delivery in low-risk, nulliparous women contemplating elective induction of labor or expectant management at 39 weeks of gestation.
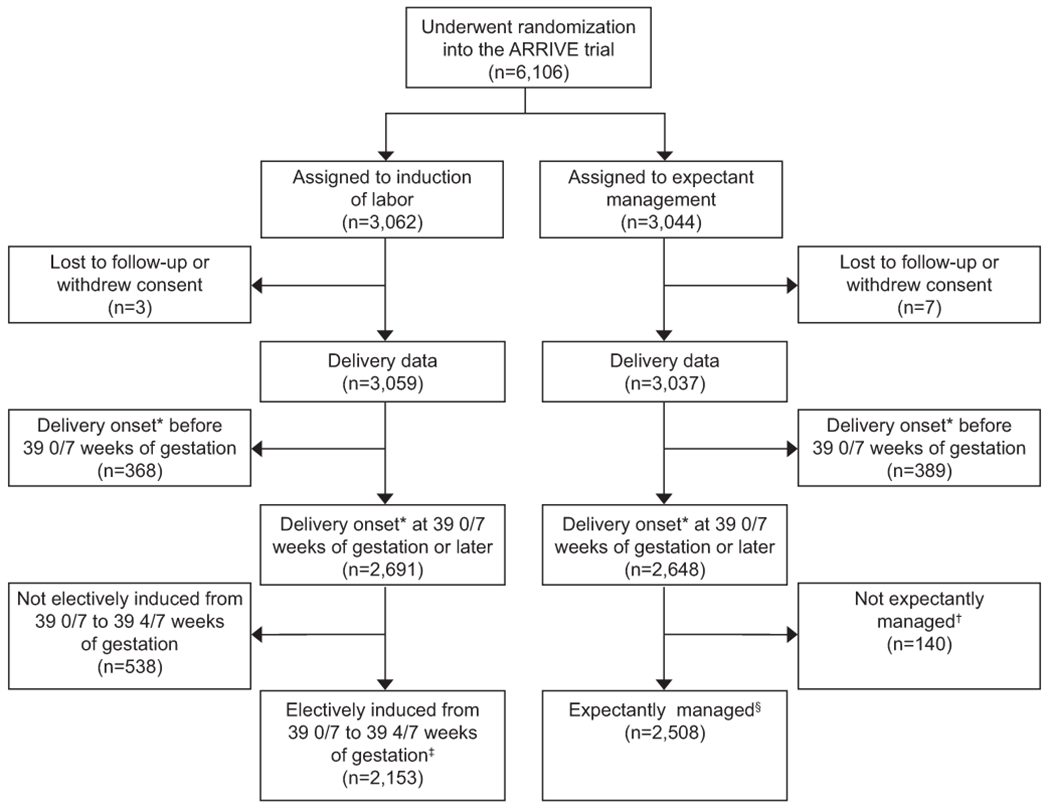
We conducted a secondary analysis of a randomized controlled trial of planned elective induction of labor at 39 weeks of gestation compared with expectant management for low-risk nulliparous women. Two groups were included for this analysis: 1) women who were randomized to the induction of labor group and underwent elective induction at 39 0/7-39 4/7 weeks of gestation and 2) women who were randomized to the expectant management group who experienced spontaneous labor or medically indicated delivery (including postterm). Multivariable logistic regression models were developed for each group using patient characteristics that would be available at the time of counseling. Model selection was based on k-fold cross-validation using backward elimination and variables that remained significant at P<.05 were retained. To compare estimated with observed rates, the elective induction of labor model was then applied to each woman in both groups to estimate individualized predicted probabilities of vaginal delivery with elective induction of labor.
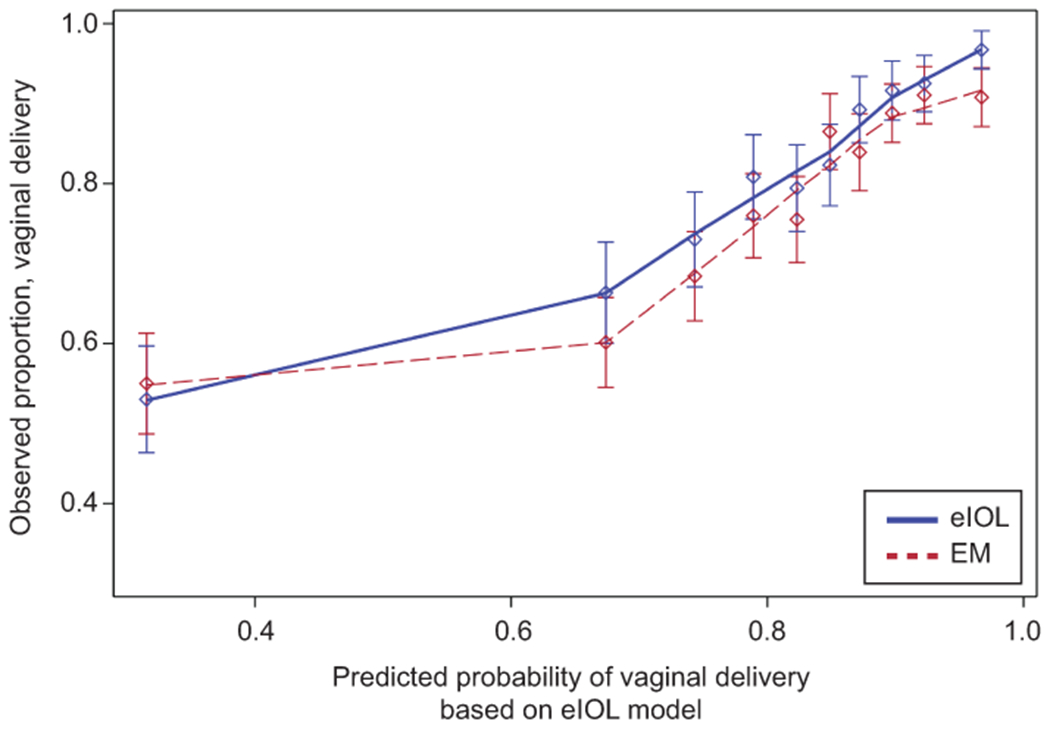
Of 6,106 women enrolled in the trial, 4,661 met criteria for this analysis. Vaginal delivery occurred in 80.6% of the 2,153 women in the elective induction of labor group and 77.2% of the 2,508 women in the expectant management group (P=.005). The final elective induction of labor model included age, height, weight, and modified Bishop score (area under the receiver operating characteristic curve [AUROC] 0.72, 95% CI 0.70-0.75). The same variables were included in the final expectant management model (AUROC 0.70, 95% CI 0.67-0.72). Across the range of predicted probability deciles derived from the elective induction of labor model, almost all women who underwent elective induction of labor at 39 weeks of gestation had a higher observed chance of vaginal delivery than expectant management.
Irrespective of the individual predicted chance of vaginal delivery from elective induction of labor at 39 weeks of gestation, vaginal delivery is generally more frequent if elective induction of labor is undertaken rather than expectant management. These data can be used to counsel nulliparous women regarding their "customized" chances of vaginal delivery as they choose between elective induction of labor or expectant management at 39 weeks of gestation.
ClinicalTrials.gov, NCT01990612.
为低危初产妇制定模型,以预测其在妊娠 39 周时选择选择性引产或期待管理的阴道分娩情况。
我们对一项比较低危初产妇妊娠 39 周时计划选择性引产与期待管理的随机对照试验进行了二次分析。本分析纳入了两组人群:1)随机分配至引产组并在妊娠 39 0/7-39 4/7 周时行选择性引产的产妇;2)随机分配至期待管理组并发生自发性临产或因医学指征行剖宫产(包括过期妊娠)的产妇。使用在咨询时可获得的患者特征为每组建立多变量逻辑回归模型。基于 K 折交叉验证,使用逐步向后消除法选择模型,并保留在 P<.05 水平有统计学意义的变量。为了比较估计值与实际值,将选择性引产模型应用于两组中的每位产妇,以估计选择性引产的个体化阴道分娩预测概率。
在参加试验的 6106 名产妇中,有 4661 名符合本分析的标准。在选择性引产组的 2153 名产妇中,80.6%行阴道分娩,在期待管理组的 2508 名产妇中,77.2%行阴道分娩(P=.005)。最终的选择性引产模型纳入了年龄、身高、体重和改良 Bishop 评分(受试者工作特征曲线下面积 [AUROC] 0.72,95%CI 0.70-0.75)。同样的变量也被纳入最终的期待管理模型(AUROC 0.70,95%CI 0.67-0.72)。在源自选择性引产模型的预测概率十分位数范围内,几乎所有在妊娠 39 周行选择性引产的产妇的实际阴道分娩机会都高于期待管理。
无论产妇在妊娠 39 周时行选择性引产的阴道分娩预测概率如何,选择性引产通常比期待管理更能增加阴道分娩的机会。这些数据可用于指导初产妇个体化选择在妊娠 39 周时行选择性引产或期待管理,使其了解自身阴道分娩的“定制”机会。
ClinicalTrials.gov,NCT01990612。