Passi-Solar Álvaro, Margozzini Paula, Mindell Jennifer S, Ruiz Milagros, Valencia-Hernandez Carlos A, Scholes Shaun
Research Department of Epidemiology and Public Health, University College London, 1-19 Torrington Place, London, WC1E 6BT, UK.
Department of Public Health, School of Medicine, Pontificia Universidad Católica de Chile, Diagonal Paraguay 362, CP 88330077, Santiago, Chile.
BMC Public Health. 2020 Sep 14;20(1):1397. doi: 10.1186/s12889-020-09483-x.
Trend data on hypertension prevalence and attainment indicators at each step of the care cascade (awareness, treatment, control) are required in Chile. This study aims to quantify trends (2003-2017) in prevalence and in the proportion of individuals with hypertension attaining each step of the care cascade among adults aged 17 years or older, and to assess the impact of lowering the blood pressure (BP) thresholds used to define elevated BP on these indicators.
We used data from 2003, 2010, and 2017 Chilean national health surveys. Each year we assessed levels of (1) mean systolic (SBP) and diastolic (DBP) blood pressure, (2) hypertension prevalence (BP ≥ 140/90 mmHg or use of antihypertensive treatment), and (3) awareness, treatment, and control. Logistic regression on pooled data was used to assess trends in binary outcomes; linear regression was used to assess trends in continuous SBP and DBP. We compared levels of hypertension prevalence using two sources to ascertain antihypertensive treatment (self-reported versus medicine inventory). The 2017 American College of Cardiology/American Heart Association (ACC/AHA) guidelines were used to re-define hypertension using lower thresholds (BP ≥ 130/80 mmHg).
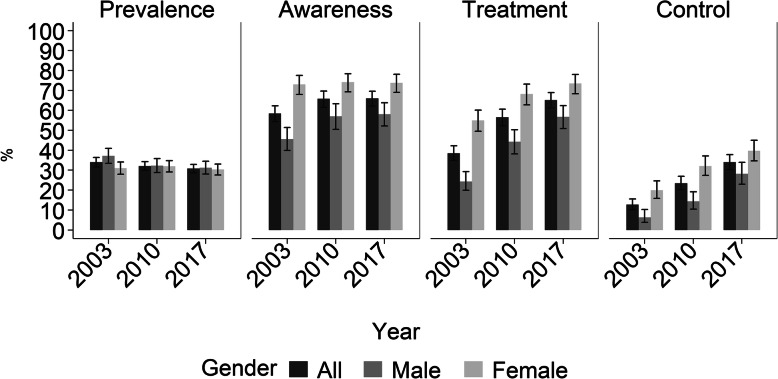
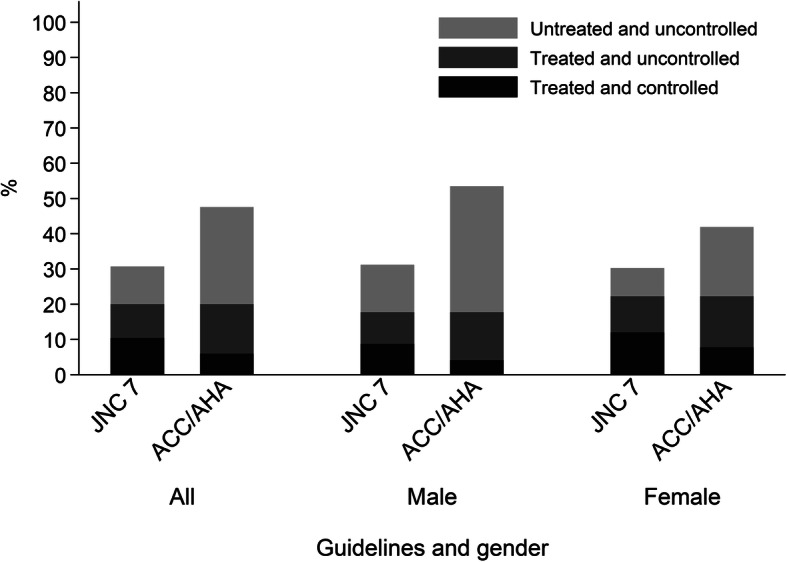
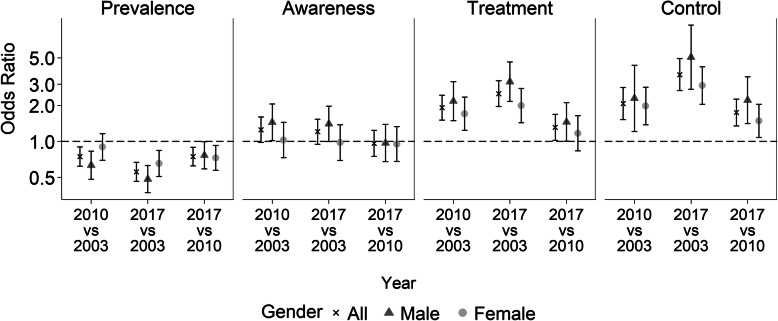
Hypertension prevalence was 34.0, 32.0 and 30.8% in 2003, 2010 and 2017, respectively. Levels of treated- and controlled-hypertension were significantly higher in 2017 than in 2003 (65% versus 41% for treatment, P < 0.001; 34% versus 14% for control, P < 0.001), while levels of awareness were stable (66% versus 59%, P = 0.130). Awareness, treatment, and control levels were higher among females in 2003, 2010, and 2017 (P < 0.001). Mean SBP and DBP decreased over the 15-year period, except for SBP among females on treatment. Adopting the 2017 ACC/AHA guidelines would increase hypertension prevalence by 17 and 55% in absolute and relative terms, respectively.
Chile has experienced a positive population-wide lowering in blood pressure distribution which may be explained partly by a significant rise in levels of treated- and controlled-hypertension since 2003. Lowering the thresholds used to define elevated BP would substantially increase the financial public health challenge of further improving attainment levels at each step of the care cascade. Innovative and collaborative strategies are needed to improve hypertension management, especially among males.
智利需要高血压患病率以及在治疗流程的每个阶段(知晓、治疗、控制)达成指标的趋势数据。本研究旨在量化17岁及以上成年人中高血压患病率以及在治疗流程各阶段达成指标的个体比例的趋势(2003 - 2017年),并评估降低用于定义血压升高的血压阈值对这些指标的影响。
我们使用了2003年、2010年和2017年智利全国健康调查的数据。每年我们评估:(1)收缩压(SBP)和舒张压(DBP)的平均水平;(2)高血压患病率(血压≥140/90 mmHg或使用抗高血压治疗);以及(3)知晓、治疗和控制情况。对汇总数据进行逻辑回归以评估二元结局的趋势;线性回归用于评估连续的收缩压和舒张压的趋势。我们使用两种确定抗高血压治疗的来源(自我报告与药品库存)比较高血压患病率水平。采用2017年美国心脏病学会/美国心脏协会(ACC/AHA)指南,使用更低的阈值(血压≥130/80 mmHg)重新定义高血压。
2003年、2010年和2017年的高血压患病率分别为34.0%、32.0%和30.8%。2017年接受治疗和控制的高血压水平显著高于2003年(治疗:65%对41%,P < 0.001;控制:34%对14%,P < 0.001),而知晓水平保持稳定(66%对59%,P = 0.130)。2003年、2010年和2017年女性的知晓、治疗和控制水平更高(P < 0.001)。在这15年期间,平均收缩压和舒张压下降,但接受治疗的女性的收缩压除外。采用2017年ACC/AHA指南将使高血压患病率在绝对值和相对值上分别增加17%和55%。
智利在全人群中经历了血压分布的积极下降,这可能部分归因于自2003年以来接受治疗和控制的高血压水平显著上升。降低用于定义血压升高的阈值将大幅增加在治疗流程各阶段进一步提高达成水平的公共卫生财政挑战。需要创新和协作策略来改善高血压管理,尤其是在男性中。